

Volume 26, Issue 4 (Winter 2026)
jrehab 2026, 26(4): 626-653 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
raheb G, Rahmani N, latifian M, Abdi K. A Conceptual Model of Rehabilitation Education in Iran Based on the Grounded Theory. jrehab 2026; 26 (4) :626-653
URL: http://rehabilitationj.uswr.ac.ir/article-1-3660-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3660-en.html



1- Substance Abuse and Dependence Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Physiotherapy, The University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,ghraheb@gmail.com
3- Department of Rehabilitation Management, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Physiotherapy, The University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
3- Department of Rehabilitation Management, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 3695 kb]
(351 Downloads)
| Abstract (HTML) (2659 Views)
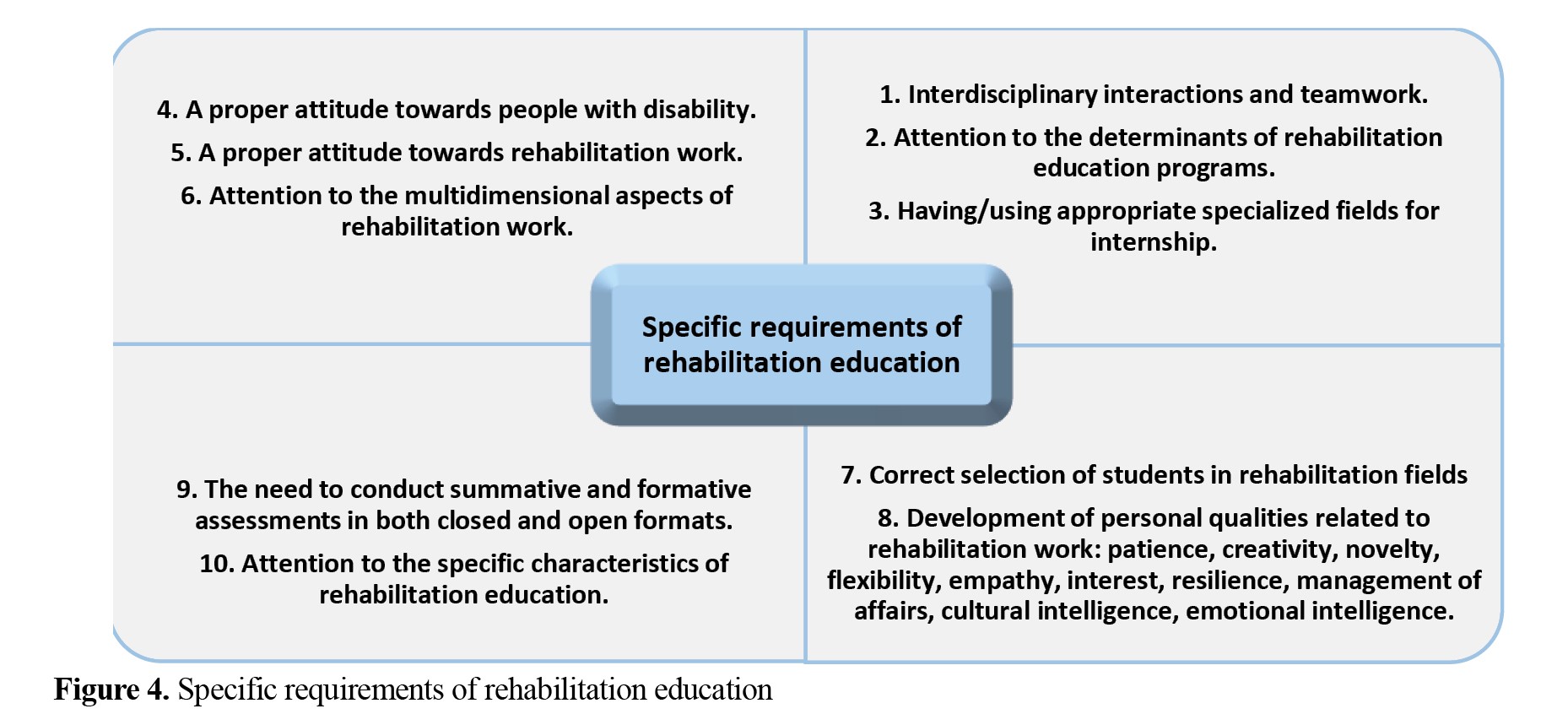
Specific requirements of rehabilitation education
Specific requirements in rehabilitation education refer to the educational mechanisms necessary for rehabilitation work. These requirements included: Interdisciplinary interactions and teamwork, attention to the determinants of rehabilitation education programs, having/using appropriate specialized fields for internship, the need to inform students about the nature of rehabilitation and the rehabilitation environments, a proper attitude towards disability and rehabilitation work, attention to the multidimensional aspects of rehabilitation work, correct selection of students in rehabilitation fields, personality of the rehabilitation specialists, the need to conduct summative and formative assessments in both closed and open formats, and instructional tools for rehabilitation education (Figure 4).
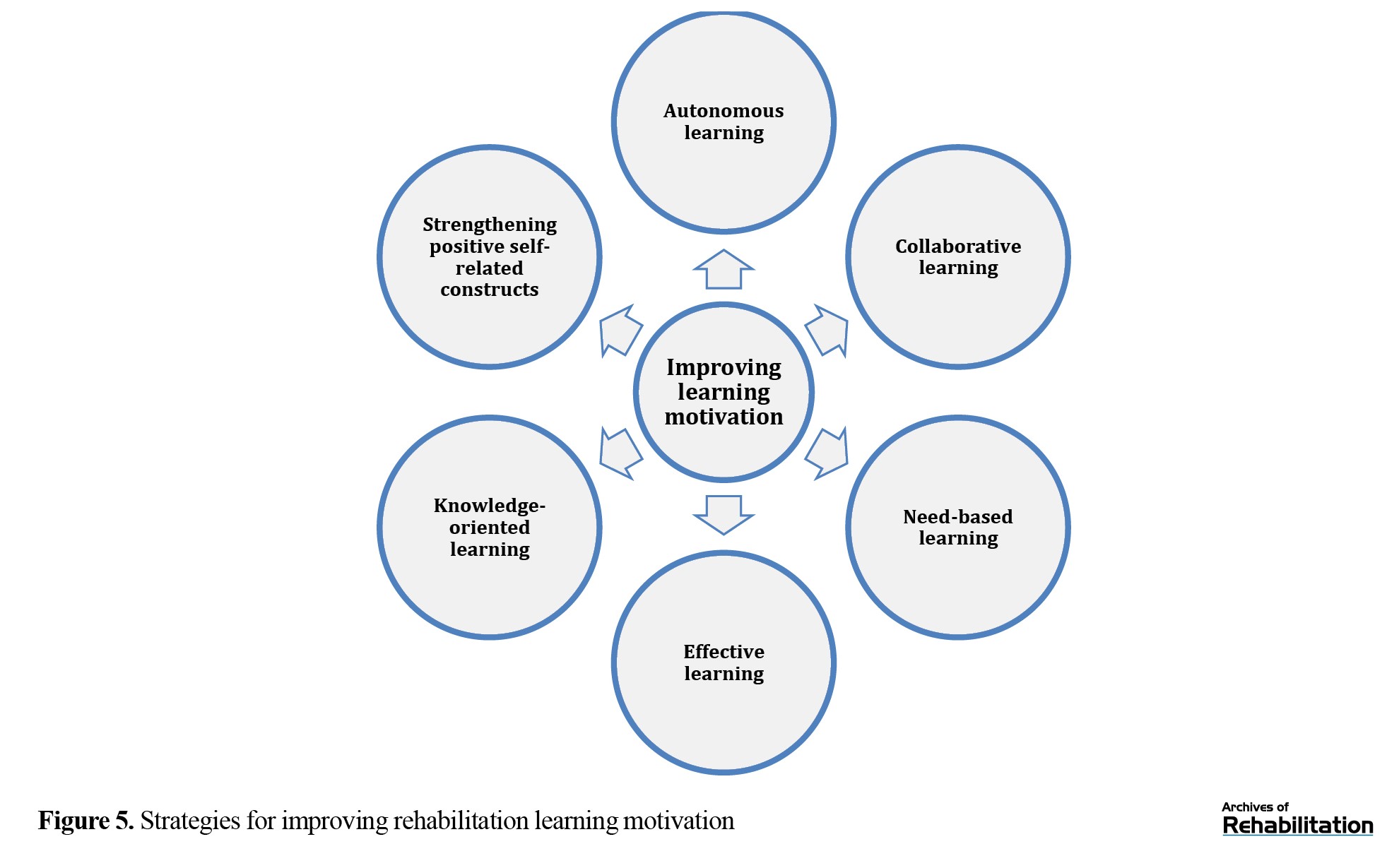
Enhancing learning motivation in rehabilitation education
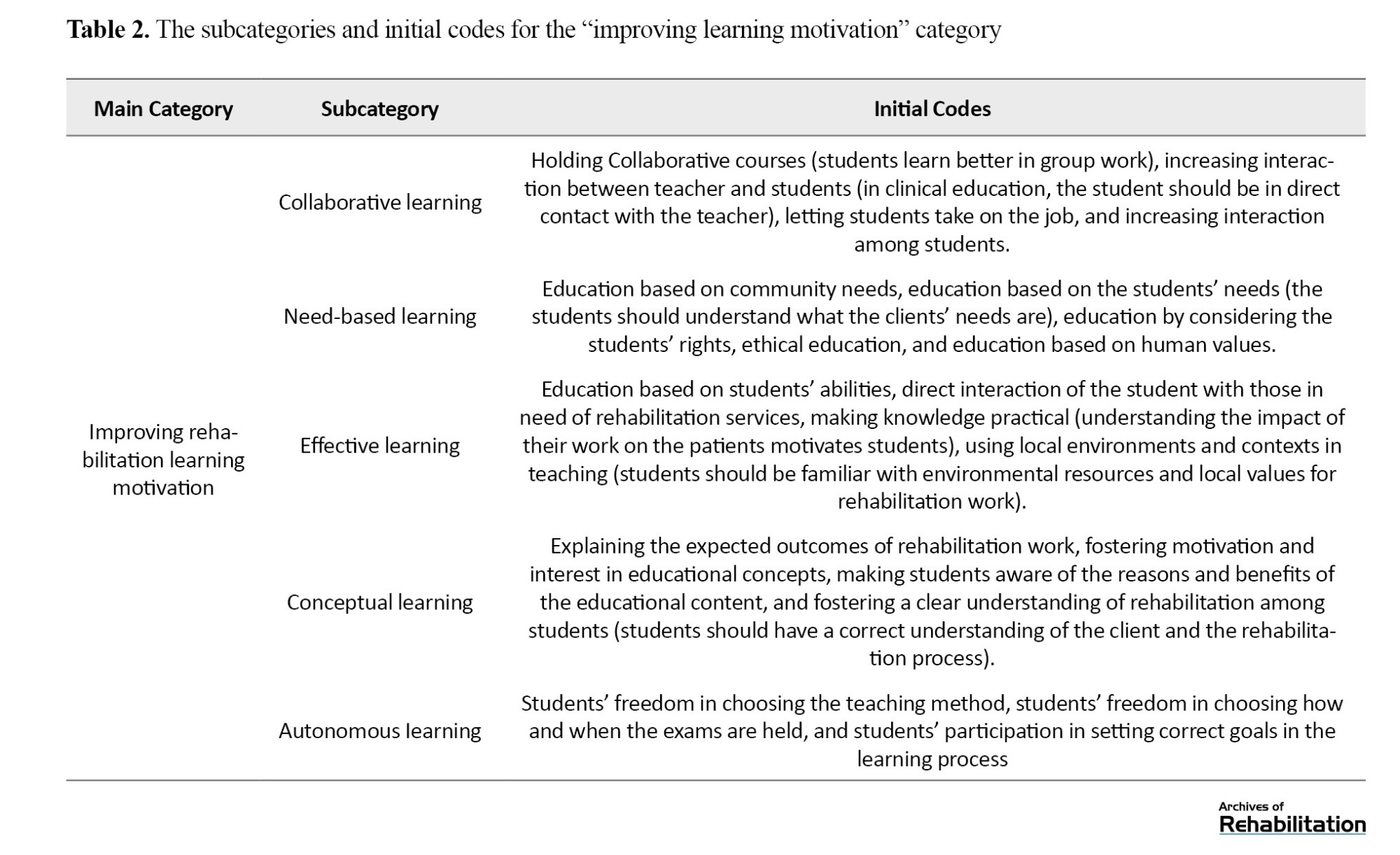
The category of improving motivation for learning rehabilitation had six sub-categories: Collaborative learning, need-based learning, effective learning, knowledge-oriented learning (education for accurate and deep understanding of concepts), autonomous learning (recognizing the student’s right to choose the study subject, process, and product), and strengthening positive self-related constructs (Figure 5).
Discussion
The goal of rehabilitation education is to educate people with specific knowledge, skills, and ideology of rehabilitation. Achieving this goal in Iran was investigated in our study with two objectives: explaining the rehabilitation education process and presenting a rehabilitation education model. The proposed model was based on the blended learning approach. In the rehabilitation education process, the use of modern teaching methods and tools is important, and the student’s skill training, skill assessment, and ability to combine skills are important indicators in rehabilitation education work. According to the research findings, collaboration between rehabilitation education stakeholders plays an effective role in improving the learning process. In the presented model, the use of collaborative learning method was an important indicator for improving learning motivation. Regarding the determinants of rehabilitation education, the model placed particular emphasis on the subject and the course of education. In this regard, the syllabus, curriculum, and components of the rehabilitation education were outlined and explained. Rehabilitation education is based on the needs of the disabled person, and is skill-based and client-centered. Rehabilitation education requires sufficient time, specific training tools, and specific human interactions, and follows specific standards.

References
Full-Text: (310 Views)
Introduction
Advancement of education in the field of rehabilitation sciences requires integrating theoretical and practical training [1]. Social accountability in rehabilitation education and medical professions is highly important [2]. To strengthen the scientific competence of rehabilitation specialists, precise planning, proper instruction, and evaluations based on the requirements of rehabilitation education should be carried out [3]. Considering developments in learning sciences, the topics related to education, and the experience of education practitioners, providing new and efficient teaching methods in the field of rehabilitation is necessary [4]. To explain the educational process, theoretical and practical dimensions and the experiences of those involved in education are essential [5]. Rehabilitation education indicators at macro and micro levels influence educational processes and outcomes. In Iran, inconsistent and limited rehabilitation policies, lack of rehabilitation education fields and facilities, and inadequate and outdated knowledge and skills of rehabilitation educators and trainers, all influence students’ learning processes. Identifying the weaknesses and strengths of rehabilitation education and the corrective suggestions made by experts in this field enables the improvement of educational quality.
The lack of learning motivation and the low scientific achievements in Iranian universities are issues that should be investigated [5]. One of the influential factors is the teaching methods used in universities. The common teaching methods applied in Iranian universities are methods in which students often have little role in the learning process [6]. In Iran, the low quality of higher education has revealed itself as a national concern for experts and researchers [7]. The issue of low motivation and academic decline in rehabilitation is also evident in medical universities. In our previous study conducted in 2013, it was found that learning motivation among students in rehabilitation sciences was below the average level [8]. The use of modern educational methods in which students play a more active role in learning can be more effective in reducing rehabilitation education problems [9]. In modern approaches, the knowledge transfer and memorization has been replaced by knowledge construction through meaningful learning. According to Givi [10], in the new millennium it is no longer possible to rely on memorization for a long time. As a result, the duties and responsibilities of professors and instructors have become heavier than before, and teacher-centered methods can no longer lead society toward complex and advanced developments [10]. Students should be active in the learning process; their learning styles, interests, and abilities should be identified, and educational programs should be designed accordingly [11], so that learners can use their learning capacities to achieve educational goals, creativity, and innovation [12]. In general, an opportunity should be provided in which learners can acquire individual skills, manage their motivation, and develop the ability to search for and integrate information to solve problems in rehabilitation topics. For this purpose, the latest technologies should be used to improve educational programs in rehabilitation [13]. Considering the existence of various philosophies, theories, and educational methods, and the specific characteristics of rehabilitation disciplines, it is necessary to achieve a theoretical consensus among professors, and theoretical and practical knowledge in order to define a theory related to rehabilitation education and present an appropriate theoretical model in this field [14]. Employing the field research method makes it possible to construct a comprehensive rehabilitation education model and achieve the mentioned goals.
It is estimated that more than 1 billion people, approximately 15% of the world’s population, live with a disability [15]. Disability is a multidimensional phenomenon encompassing physical health, personal/environmental factors, inaccessible infrastructure, social misconceptions, discrimination, and insufficient social support [16]. Rehabilitation consists of exercises that compensate for functional loss as much as possible and, on the other hand, facilitate social adaptation [17]. In rehabilitation education, the overarching rehabilitation policies influence the processes and outcomes of education and affect the knowledge and skills of students [18, 19].
Education in rehabilitation sciences is intertwined with principles based on knowledge, skill, and techniques for establishing effective communication with people. These techniques are influential factors in rehabilitation and in achieving the goals of rehabilitation science. In rehabilitation intervention, linking evidence to rehabilitation services in clinical practice is essential. In teaching rehabilitation interventions, elements such as Collaborative learning, educational framing, thinking about the teaching–learning process, and the necessity of connecting theory to practice are among the fundamental indicators in rehabilitation education. In rehabilitation teaching models, emphasis is placed on fostering accurate conceptual understanding, developing clinical competencies, maximizing the use of educational opportunities, planning effective internships, providing appropriate student support, and allowing students to have autonomy in the educational process [20].
There are a few studies in the field of rehabilitation education in Iran. The distinctive nature of rehabilitation (underlying beliefs) and its educational requirements (methods, tools, and facilities necessary for effective training) warrant further investigations. This study seeks to address the following questions: How is the rehabilitation education process? and what conceptual model best represents rehabilitation education? Using a grounded theory approach, this study aims to develop a context-specific and practical model for both theoretical and practical rehabilitation education based on the perspectives of individuals directly involved in rehabilitation education.
Materials and Methods
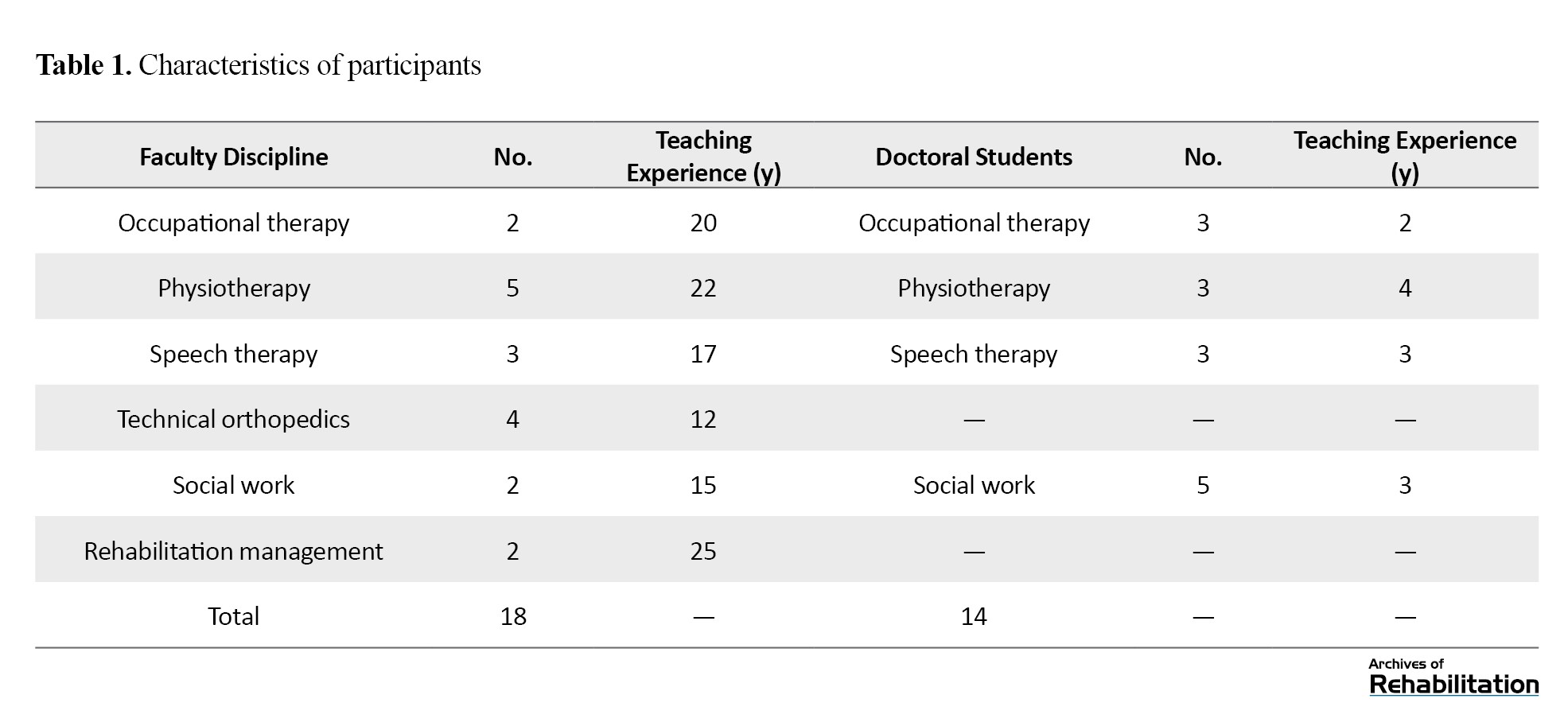
This study was conducted using a grounded theory approach. Participants included faculty members and doctoral students in rehabilitation sciences from the University of Social Welfare and Rehabilitation Sciences. Sampling was done using a purposive method. Sampling continued until data saturation, which was achieved after 32 interviews. The inclusion criteria for faculty members included at least five years of teaching experience related to rehabilitation courses and willingness to participate in the study. The Inclusion criteria for students were the study or teaching experience in one of the rehabilitation disciplines, as well as willingness to participate in the study. The faculty members included two occupational therapists with 20 years of teaching experience, five physiotherapists with 22 years of teaching experience, three speech-language therapists with 17 years of experience, two social workers with 15 years of experience, two rehabilitation management specialists with 25 years of experience, and four prosthetics and orthotics specialists with 12 years of teaching experience. In addition, 14 doctoral students in occupational therapy, speech therapy, and physiotherapy were included in the study.
Data were collected through semi-structured interviews focused on key components of rehabilitation education. To minimize the influence of pre-existing theoretical frameworks and support the emergence of original findings, the interview guide was developed based on preliminary interviews with faculty members and students in rehabilitation sciences. The final interview questions were reviewed and validated by an expert panel. Interview topics addressed participants’ experiences with teaching rehabilitation content in both theoretical and practical course, the structures and processes of rehabilitation education, instructional teaching models and skills, supervision and evaluation practices, interpersonal relationships among educational stakeholders, distinctive characteristics of rehabilitation education, strengths and challenges in current educational practices, examples of effective rehabilitation teaching experiences, factors influencing student motivation, commonly used rehabilitation teaching methods and their strengths and limitations; and suggestions for improving rehabilitation education. Interviews were conducted by the researcher with the assistance of a faculty member in the field of rehabilitation (social work). Each interview lasted approximately 45 minutes. The interviews with faculty members were held in their university offices, while interviews with doctoral students were done in their academic departments. Before audio recording, all participants were fully informed about the recording procedure and provided consent.
For data analysis, audio recordings were transcribed verbatim and reviewed multiple times to achieve familiarity with the data. Analysis was done based on Corbin and Strauss’s grounded theory method. Semantic units were identified and condensed; initial codes were generated and refined, and semantic comparisons were conducted to identify similarities and differences. Related codes were grouped into higher-level categories through an iterative inductive and deductive process. Constant comparison of subcategories led to the development of analytically coherent categories. All coding and analytical procedures were conducted manually. To enhance the rigor and trustworthiness of the findings, the researcher employed prolonged engagement with the data, allocated sufficient time for data collection and analysis, maintained continuous presence in the research setting, shared preliminary findings with participants for confirmation, collected data from diverse stakeholders, and actively sought disconfirming cases and alternative interpretations.
Results
Table 1 presents the characteristics of participants.
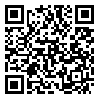
Based on the study findings, seven core categories of rehabilitation education were identified, as illustrated in Figure 1.
Advancement of education in the field of rehabilitation sciences requires integrating theoretical and practical training [1]. Social accountability in rehabilitation education and medical professions is highly important [2]. To strengthen the scientific competence of rehabilitation specialists, precise planning, proper instruction, and evaluations based on the requirements of rehabilitation education should be carried out [3]. Considering developments in learning sciences, the topics related to education, and the experience of education practitioners, providing new and efficient teaching methods in the field of rehabilitation is necessary [4]. To explain the educational process, theoretical and practical dimensions and the experiences of those involved in education are essential [5]. Rehabilitation education indicators at macro and micro levels influence educational processes and outcomes. In Iran, inconsistent and limited rehabilitation policies, lack of rehabilitation education fields and facilities, and inadequate and outdated knowledge and skills of rehabilitation educators and trainers, all influence students’ learning processes. Identifying the weaknesses and strengths of rehabilitation education and the corrective suggestions made by experts in this field enables the improvement of educational quality.
The lack of learning motivation and the low scientific achievements in Iranian universities are issues that should be investigated [5]. One of the influential factors is the teaching methods used in universities. The common teaching methods applied in Iranian universities are methods in which students often have little role in the learning process [6]. In Iran, the low quality of higher education has revealed itself as a national concern for experts and researchers [7]. The issue of low motivation and academic decline in rehabilitation is also evident in medical universities. In our previous study conducted in 2013, it was found that learning motivation among students in rehabilitation sciences was below the average level [8]. The use of modern educational methods in which students play a more active role in learning can be more effective in reducing rehabilitation education problems [9]. In modern approaches, the knowledge transfer and memorization has been replaced by knowledge construction through meaningful learning. According to Givi [10], in the new millennium it is no longer possible to rely on memorization for a long time. As a result, the duties and responsibilities of professors and instructors have become heavier than before, and teacher-centered methods can no longer lead society toward complex and advanced developments [10]. Students should be active in the learning process; their learning styles, interests, and abilities should be identified, and educational programs should be designed accordingly [11], so that learners can use their learning capacities to achieve educational goals, creativity, and innovation [12]. In general, an opportunity should be provided in which learners can acquire individual skills, manage their motivation, and develop the ability to search for and integrate information to solve problems in rehabilitation topics. For this purpose, the latest technologies should be used to improve educational programs in rehabilitation [13]. Considering the existence of various philosophies, theories, and educational methods, and the specific characteristics of rehabilitation disciplines, it is necessary to achieve a theoretical consensus among professors, and theoretical and practical knowledge in order to define a theory related to rehabilitation education and present an appropriate theoretical model in this field [14]. Employing the field research method makes it possible to construct a comprehensive rehabilitation education model and achieve the mentioned goals.
It is estimated that more than 1 billion people, approximately 15% of the world’s population, live with a disability [15]. Disability is a multidimensional phenomenon encompassing physical health, personal/environmental factors, inaccessible infrastructure, social misconceptions, discrimination, and insufficient social support [16]. Rehabilitation consists of exercises that compensate for functional loss as much as possible and, on the other hand, facilitate social adaptation [17]. In rehabilitation education, the overarching rehabilitation policies influence the processes and outcomes of education and affect the knowledge and skills of students [18, 19].
Education in rehabilitation sciences is intertwined with principles based on knowledge, skill, and techniques for establishing effective communication with people. These techniques are influential factors in rehabilitation and in achieving the goals of rehabilitation science. In rehabilitation intervention, linking evidence to rehabilitation services in clinical practice is essential. In teaching rehabilitation interventions, elements such as Collaborative learning, educational framing, thinking about the teaching–learning process, and the necessity of connecting theory to practice are among the fundamental indicators in rehabilitation education. In rehabilitation teaching models, emphasis is placed on fostering accurate conceptual understanding, developing clinical competencies, maximizing the use of educational opportunities, planning effective internships, providing appropriate student support, and allowing students to have autonomy in the educational process [20].
There are a few studies in the field of rehabilitation education in Iran. The distinctive nature of rehabilitation (underlying beliefs) and its educational requirements (methods, tools, and facilities necessary for effective training) warrant further investigations. This study seeks to address the following questions: How is the rehabilitation education process? and what conceptual model best represents rehabilitation education? Using a grounded theory approach, this study aims to develop a context-specific and practical model for both theoretical and practical rehabilitation education based on the perspectives of individuals directly involved in rehabilitation education.
Materials and Methods
This study was conducted using a grounded theory approach. Participants included faculty members and doctoral students in rehabilitation sciences from the University of Social Welfare and Rehabilitation Sciences. Sampling was done using a purposive method. Sampling continued until data saturation, which was achieved after 32 interviews. The inclusion criteria for faculty members included at least five years of teaching experience related to rehabilitation courses and willingness to participate in the study. The Inclusion criteria for students were the study or teaching experience in one of the rehabilitation disciplines, as well as willingness to participate in the study. The faculty members included two occupational therapists with 20 years of teaching experience, five physiotherapists with 22 years of teaching experience, three speech-language therapists with 17 years of experience, two social workers with 15 years of experience, two rehabilitation management specialists with 25 years of experience, and four prosthetics and orthotics specialists with 12 years of teaching experience. In addition, 14 doctoral students in occupational therapy, speech therapy, and physiotherapy were included in the study.
Data were collected through semi-structured interviews focused on key components of rehabilitation education. To minimize the influence of pre-existing theoretical frameworks and support the emergence of original findings, the interview guide was developed based on preliminary interviews with faculty members and students in rehabilitation sciences. The final interview questions were reviewed and validated by an expert panel. Interview topics addressed participants’ experiences with teaching rehabilitation content in both theoretical and practical course, the structures and processes of rehabilitation education, instructional teaching models and skills, supervision and evaluation practices, interpersonal relationships among educational stakeholders, distinctive characteristics of rehabilitation education, strengths and challenges in current educational practices, examples of effective rehabilitation teaching experiences, factors influencing student motivation, commonly used rehabilitation teaching methods and their strengths and limitations; and suggestions for improving rehabilitation education. Interviews were conducted by the researcher with the assistance of a faculty member in the field of rehabilitation (social work). Each interview lasted approximately 45 minutes. The interviews with faculty members were held in their university offices, while interviews with doctoral students were done in their academic departments. Before audio recording, all participants were fully informed about the recording procedure and provided consent.
For data analysis, audio recordings were transcribed verbatim and reviewed multiple times to achieve familiarity with the data. Analysis was done based on Corbin and Strauss’s grounded theory method. Semantic units were identified and condensed; initial codes were generated and refined, and semantic comparisons were conducted to identify similarities and differences. Related codes were grouped into higher-level categories through an iterative inductive and deductive process. Constant comparison of subcategories led to the development of analytically coherent categories. All coding and analytical procedures were conducted manually. To enhance the rigor and trustworthiness of the findings, the researcher employed prolonged engagement with the data, allocated sufficient time for data collection and analysis, maintained continuous presence in the research setting, shared preliminary findings with participants for confirmation, collected data from diverse stakeholders, and actively sought disconfirming cases and alternative interpretations.
Results
Table 1 presents the characteristics of participants.
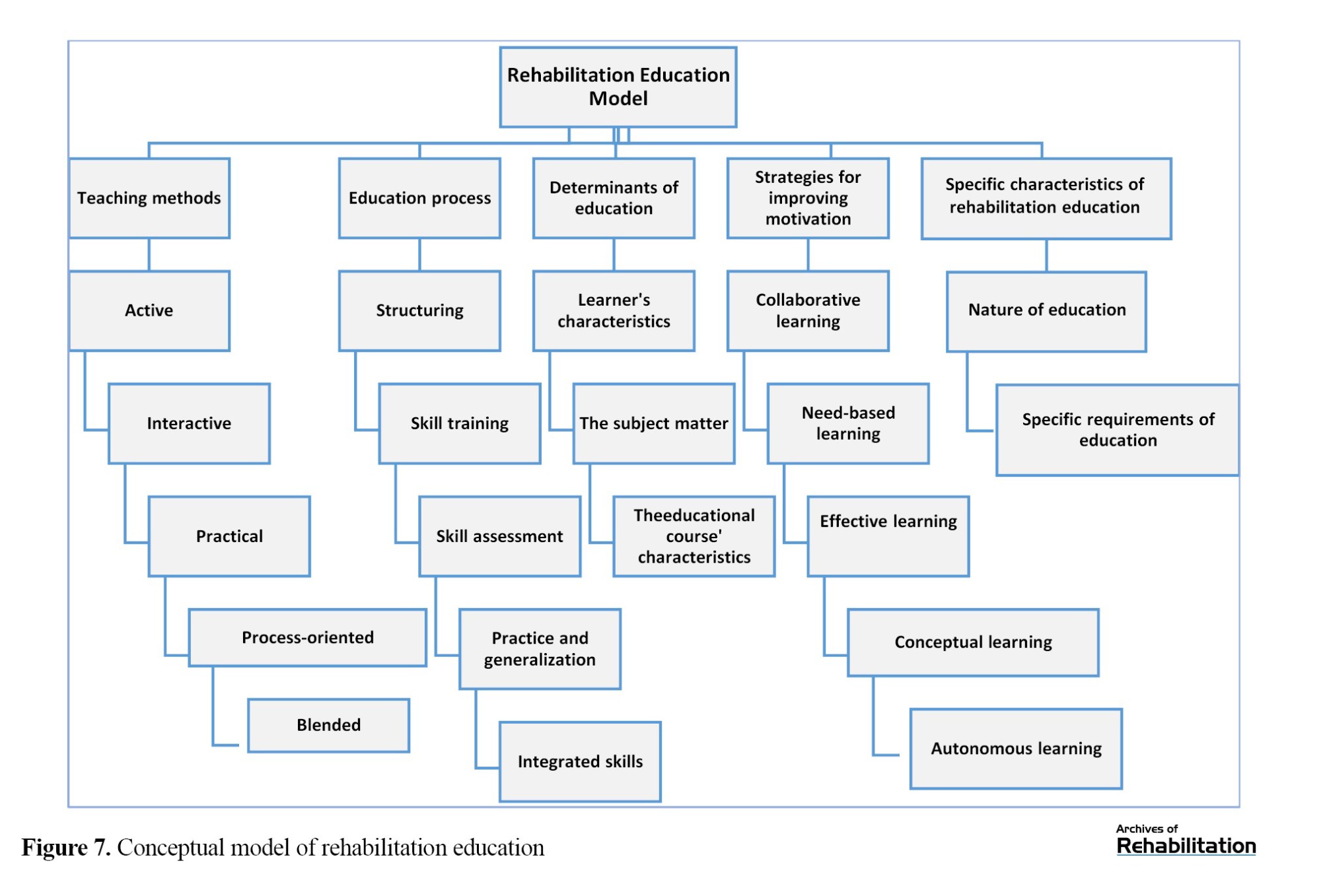
Based on the study findings, seven core categories of rehabilitation education were identified, as illustrated in Figure 1.
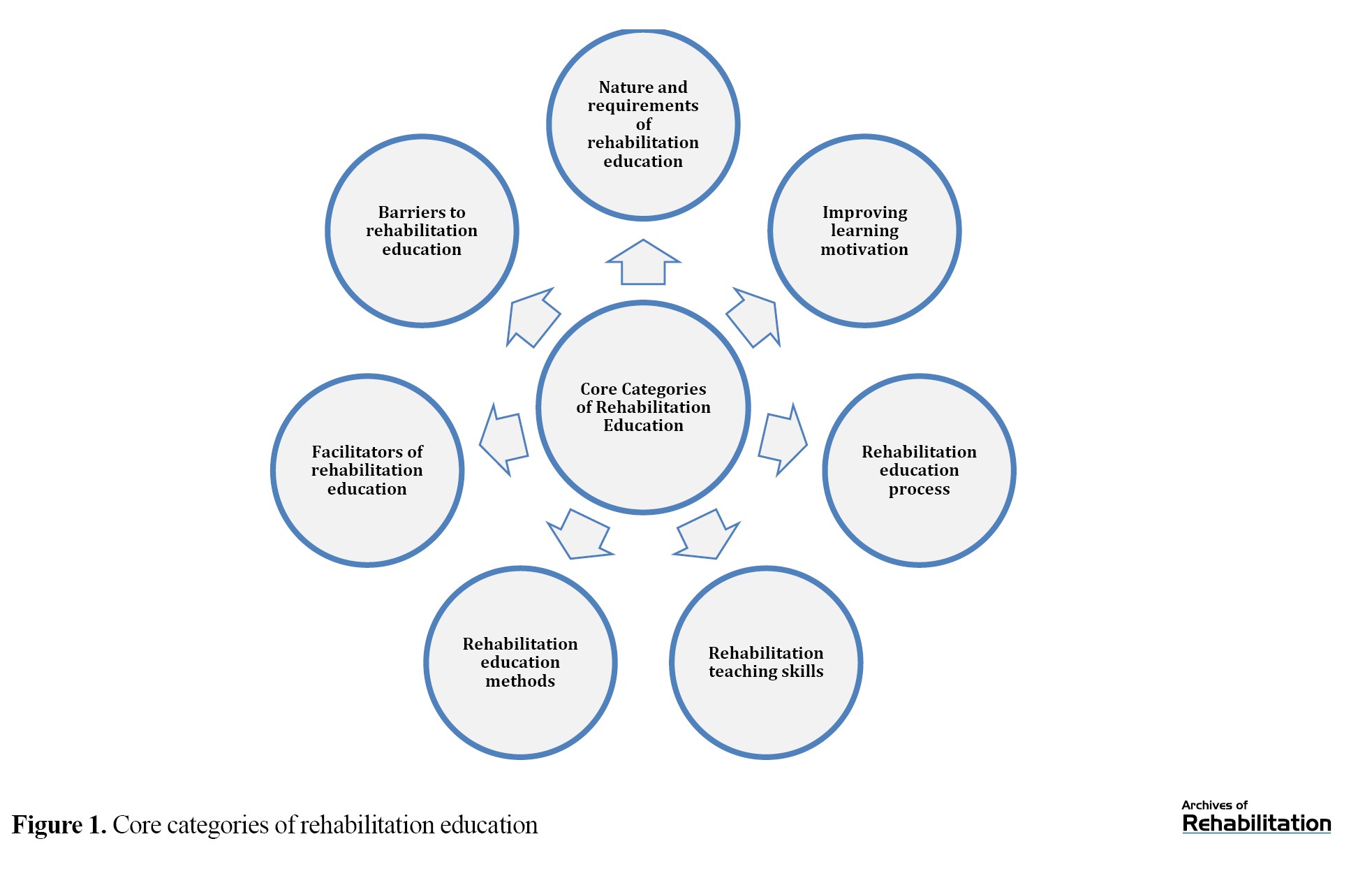
These categories emerged from integrating initial categories and subcategories and represent the overall model of rehabilitation education. Among them, the nature and requirements of rehabilitation education reflect the underlying philosophical foundations of rehabilitation teaching and define the mechanisms essential for effective training. This construct was identified as the study’s central variable. It interacts reciprocally with other categories (Figure 2).
The conceptual paradigms derived from the analysis in this study were organized based on this central category. In this model, the nature and requirements of rehabilitation education included the components, mediating factors, and outcomes of rehabilitation education.
Nature of rehabilitation education
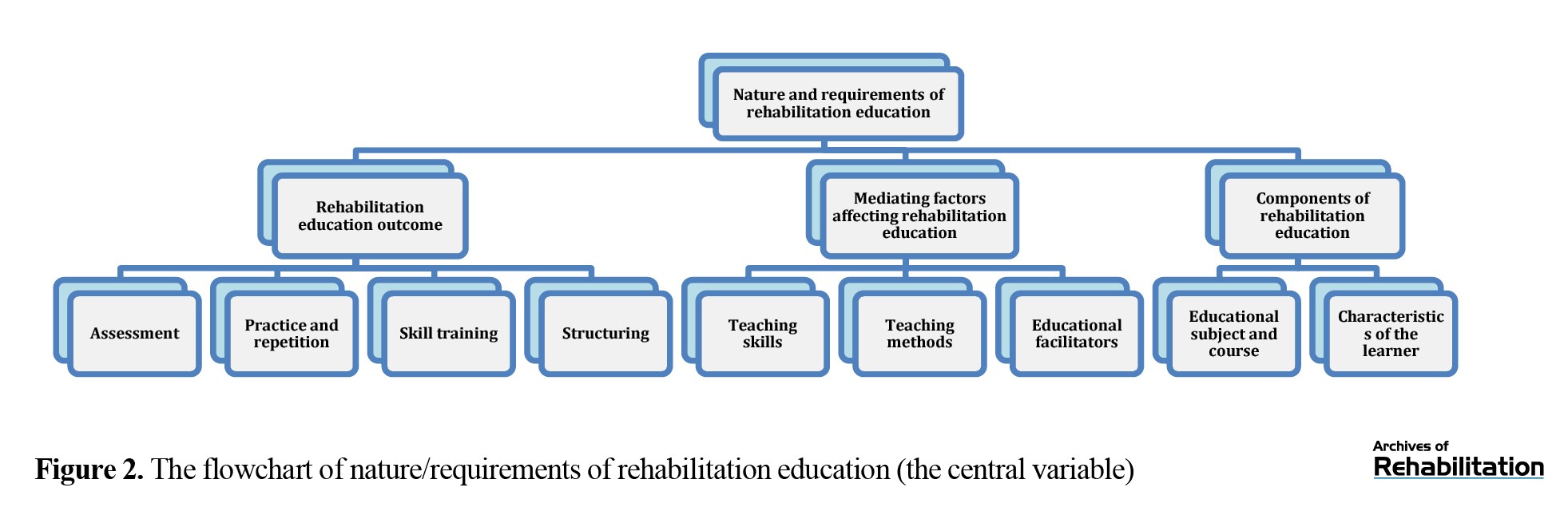
Rehabilitation education considers rehabilitation as a philosophy of life. As one faculty member stated: “The rehabilitation process encompasses all aspects of a disabled person’s life”. Another faculty member argued: “There cannot and should not be a one-size-fits-all prescription for rehabilitation; the treatment plan varies from person to person.” Accordingly, rehabilitation education requires that each client be engaged in rehabilitation programs with careful attention to individual characteristics. From this perspective, rehabilitation is a multidimensional process aimed at addressing the complex needs of clients. Another defining feature of rehabilitation was the uncertainty of evidence and its dependence on context, culture, and social capital. As one faculty member explained, “In rehabilitation, rehabilitation methods have a relative effect on different clients, and the certainty of the effectiveness of interventions cannot be proven.” Figure 3 illustrates the constructs of rehabilitation education.
Nature of rehabilitation education
Rehabilitation education considers rehabilitation as a philosophy of life. As one faculty member stated: “The rehabilitation process encompasses all aspects of a disabled person’s life”. Another faculty member argued: “There cannot and should not be a one-size-fits-all prescription for rehabilitation; the treatment plan varies from person to person.” Accordingly, rehabilitation education requires that each client be engaged in rehabilitation programs with careful attention to individual characteristics. From this perspective, rehabilitation is a multidimensional process aimed at addressing the complex needs of clients. Another defining feature of rehabilitation was the uncertainty of evidence and its dependence on context, culture, and social capital. As one faculty member explained, “In rehabilitation, rehabilitation methods have a relative effect on different clients, and the certainty of the effectiveness of interventions cannot be proven.” Figure 3 illustrates the constructs of rehabilitation education.
Specific requirements of rehabilitation education
Specific requirements in rehabilitation education refer to the educational mechanisms necessary for rehabilitation work. These requirements included: Interdisciplinary interactions and teamwork, attention to the determinants of rehabilitation education programs, having/using appropriate specialized fields for internship, the need to inform students about the nature of rehabilitation and the rehabilitation environments, a proper attitude towards disability and rehabilitation work, attention to the multidimensional aspects of rehabilitation work, correct selection of students in rehabilitation fields, personality of the rehabilitation specialists, the need to conduct summative and formative assessments in both closed and open formats, and instructional tools for rehabilitation education (Figure 4).
Enhancing learning motivation in rehabilitation education
The category of improving motivation for learning rehabilitation had six sub-categories: Collaborative learning, need-based learning, effective learning, knowledge-oriented learning (education for accurate and deep understanding of concepts), autonomous learning (recognizing the student’s right to choose the study subject, process, and product), and strengthening positive self-related constructs (Figure 5).
Learning motivation is a key factor in effective learning. Learners require a driving force to guide their learning process, and this force comes from the learner’s internal and external motivations. Intrinsic motivation, regardless of external factors, is a strong indicator in advancing the learning process. Intrinsic motivation arises from the learners’ internal needs and understanding the effectiveness of what they have learned. Learners’ participation in the learning process and their freedom to choose the components of education are effective factors in improving learning motivation. Regarding Collaborative learning, one student stated: “When we work together in both theoretical and practical tasks, we are more interested in doing the work.” Regarding autonomous learning, one student argued: “I don’t feel good about mandatory courses that is pre-written from start to end.” Higher levels of self-concept, self-efficacy, and self-regulation in learners were also found to be effective in learning motivation. As one faculty member explained, “The better a student self-assesses their ability to do a task, the better they will do it.” Table 2 summarizes the subcategories and their initial codes that contribute to enhancing rehabilitation learning motivation.
The rehabilitation education process
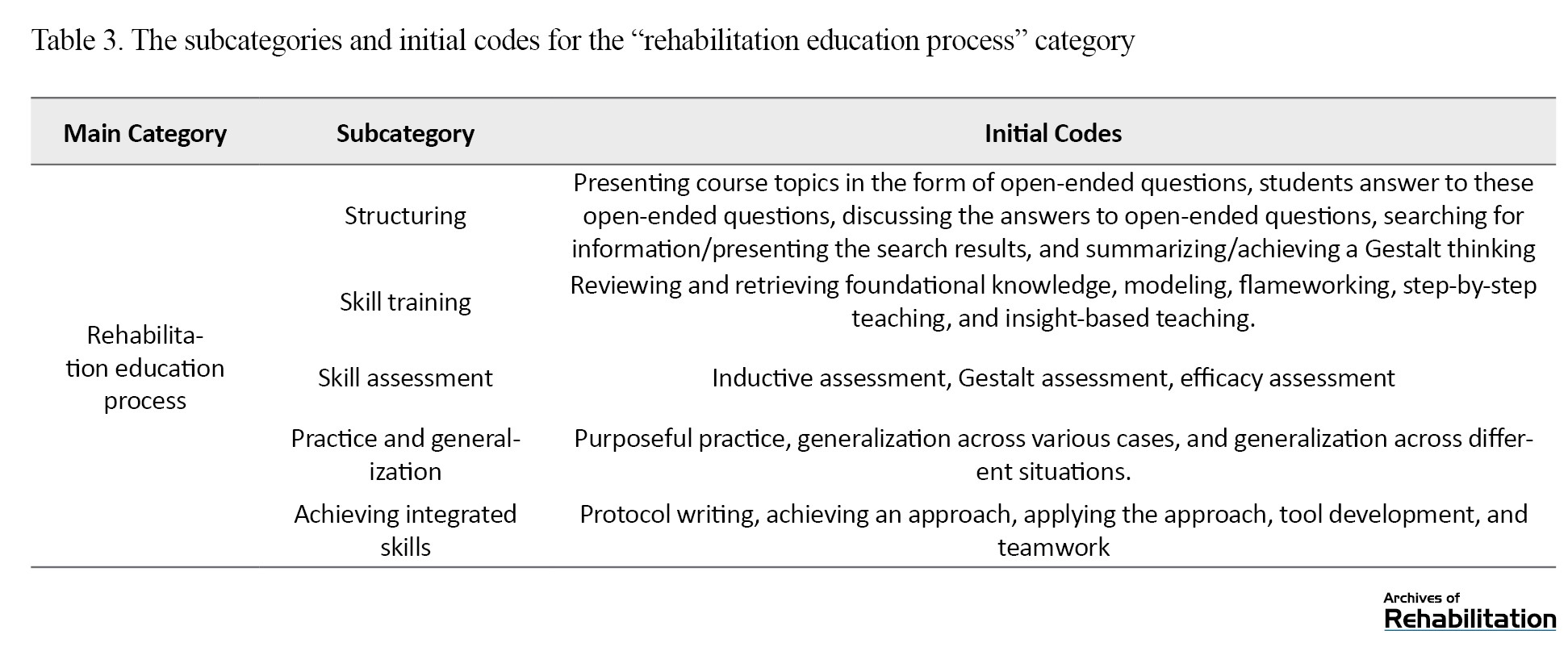
The rehabilitation education process occurs during the training period. To purposefully advance the learning process in line with the intended educational philosophy, instructors should structure the initiation, guidance, and assessment of classroom activities. They should also have sufficient mastery of educational skills, how to teach skills, and how to evaluate them, and design a written plan for repeating and practicing skills. In addition, they should help the student achieve the ability to integrate these skills. Table 3 summarizes the subcategories and their initial codes that contribute to the process of rehabilitation education.
Rehabilitation teaching skills
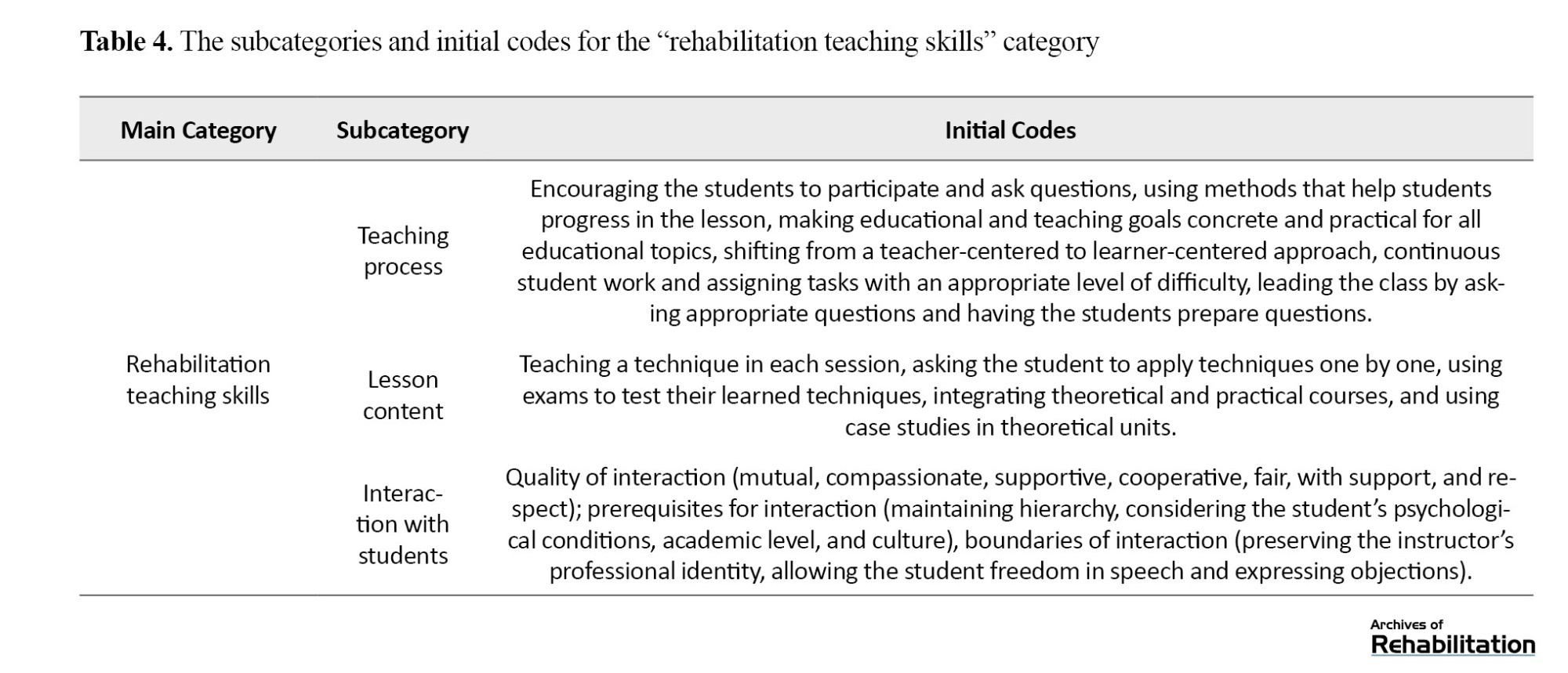
The instructor should be able to apply teaching skills throughout the teaching process and at its various stages. According to the “rehabilitation teaching skills” category, the instructor should be equipped with skills, outlined in Table 4, for teaching rehabilitation, developing educational content, and communicating with the students.
Rehabilitation teaching methods
Rehabilitation teaching methods were classified into five subcategories: active teaching, interactive teaching, practical teaching, process-oriented teaching, and blended teaching methods (Table 5).
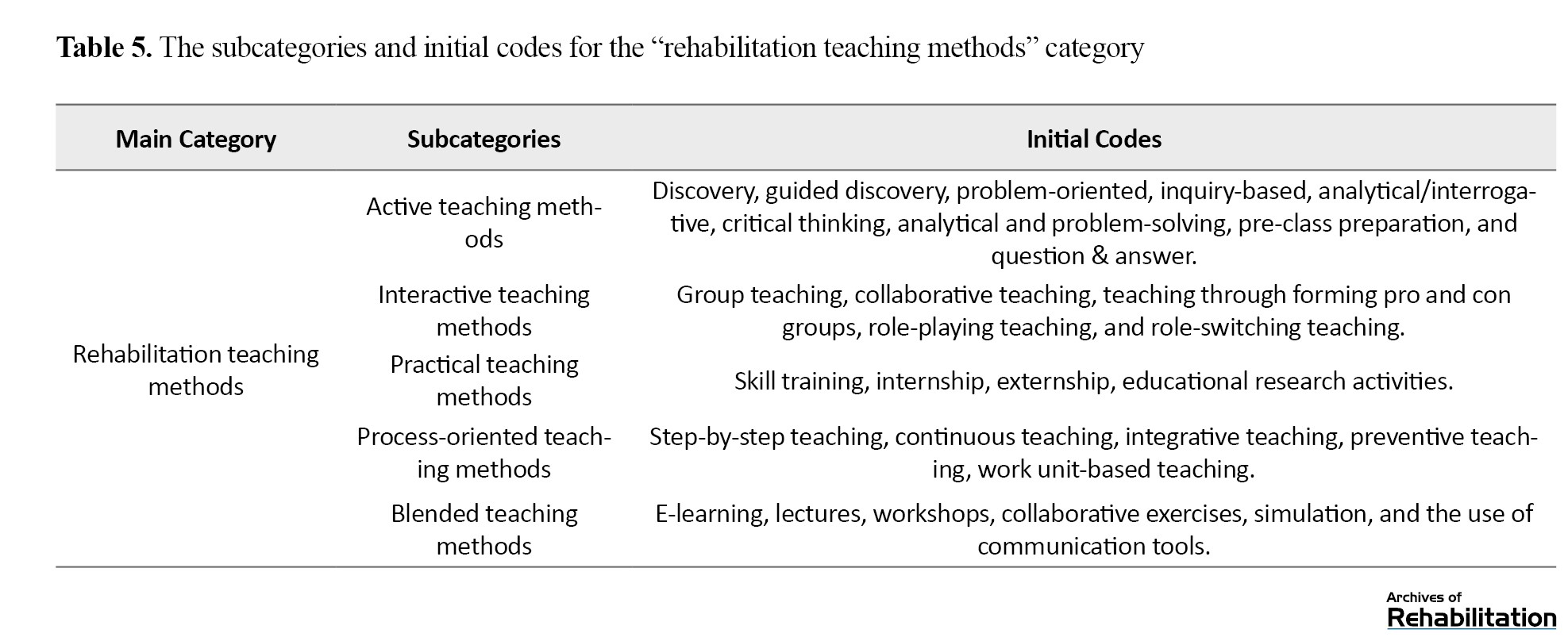
The teaching methods are indirect, learner-centered instructional approaches, in which interactive, practical teaching plays a key role. In these teaching methods, particular emphasis is placed on the learning process and its progression, as well as on the integrated use of multiple tools and active instructional strategies.
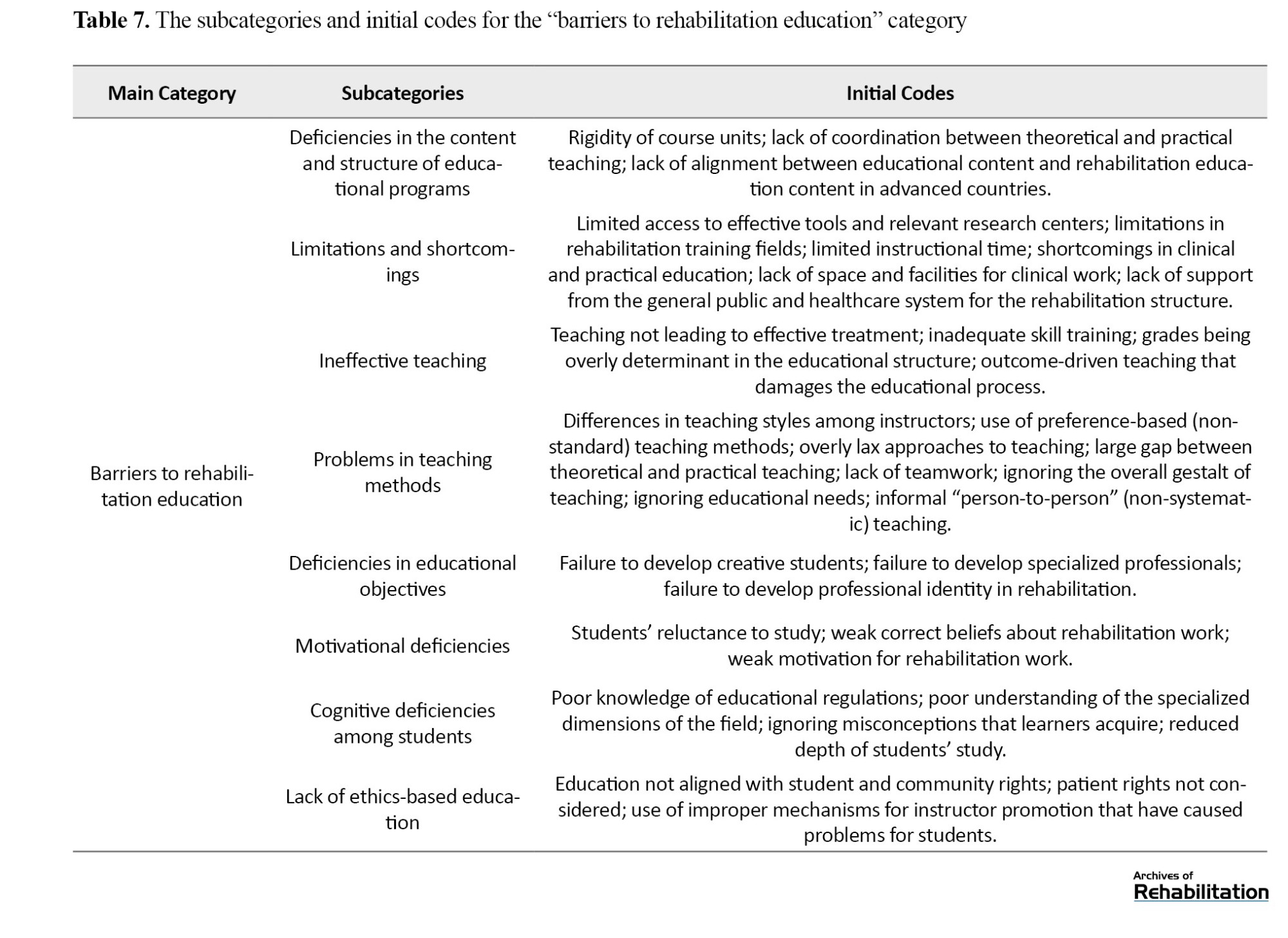
Facilitating and inhibiting factors in rehabilitation education
The use of up-to-date and efficient educational tools, the instructor’s ability in teaching, presentation of effective educational models, periodic and comprehensive evaluations, and supportive, professional, and warm instructor–student interactions were among the factors that facilitate rehabilitation education. In contrast, ineffective and inefficient teaching, deficiencies in educational content and objectives, lack of student motivation, insufficient knowledge, and the lack of ethics-based teaching were barriers to rehabilitation education (Table 6).
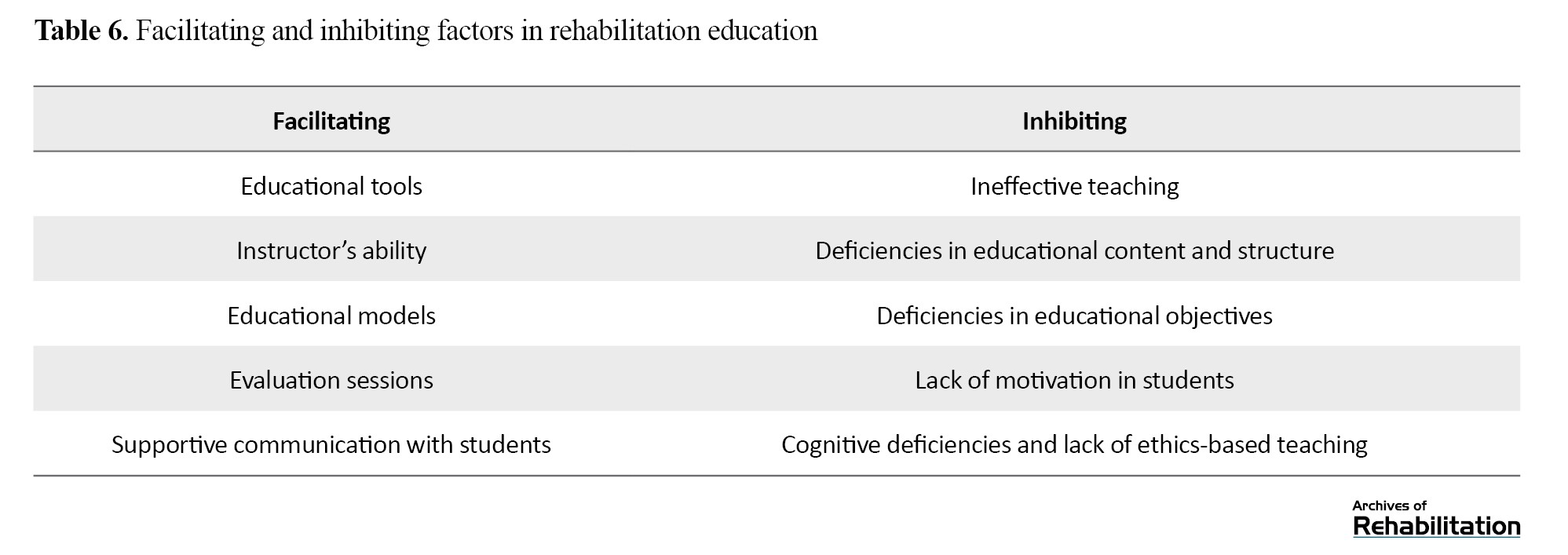
Table 7 summarizes the initial codes that contribute to the barriers to rehabilitation education.
The rehabilitation education process
The rehabilitation education process occurs during the training period. To purposefully advance the learning process in line with the intended educational philosophy, instructors should structure the initiation, guidance, and assessment of classroom activities. They should also have sufficient mastery of educational skills, how to teach skills, and how to evaluate them, and design a written plan for repeating and practicing skills. In addition, they should help the student achieve the ability to integrate these skills. Table 3 summarizes the subcategories and their initial codes that contribute to the process of rehabilitation education.
Rehabilitation teaching skills
The instructor should be able to apply teaching skills throughout the teaching process and at its various stages. According to the “rehabilitation teaching skills” category, the instructor should be equipped with skills, outlined in Table 4, for teaching rehabilitation, developing educational content, and communicating with the students.
Rehabilitation teaching methods
Rehabilitation teaching methods were classified into five subcategories: active teaching, interactive teaching, practical teaching, process-oriented teaching, and blended teaching methods (Table 5).
The teaching methods are indirect, learner-centered instructional approaches, in which interactive, practical teaching plays a key role. In these teaching methods, particular emphasis is placed on the learning process and its progression, as well as on the integrated use of multiple tools and active instructional strategies.
Facilitating and inhibiting factors in rehabilitation education
The use of up-to-date and efficient educational tools, the instructor’s ability in teaching, presentation of effective educational models, periodic and comprehensive evaluations, and supportive, professional, and warm instructor–student interactions were among the factors that facilitate rehabilitation education. In contrast, ineffective and inefficient teaching, deficiencies in educational content and objectives, lack of student motivation, insufficient knowledge, and the lack of ethics-based teaching were barriers to rehabilitation education (Table 6).
Table 7 summarizes the initial codes that contribute to the barriers to rehabilitation education.
Discussion
The goal of rehabilitation education is to educate people with specific knowledge, skills, and ideology of rehabilitation. Achieving this goal in Iran was investigated in our study with two objectives: explaining the rehabilitation education process and presenting a rehabilitation education model. The proposed model was based on the blended learning approach. In the rehabilitation education process, the use of modern teaching methods and tools is important, and the student’s skill training, skill assessment, and ability to combine skills are important indicators in rehabilitation education work. According to the research findings, collaboration between rehabilitation education stakeholders plays an effective role in improving the learning process. In the presented model, the use of collaborative learning method was an important indicator for improving learning motivation. Regarding the determinants of rehabilitation education, the model placed particular emphasis on the subject and the course of education. In this regard, the syllabus, curriculum, and components of the rehabilitation education were outlined and explained. Rehabilitation education is based on the needs of the disabled person, and is skill-based and client-centered. Rehabilitation education requires sufficient time, specific training tools, and specific human interactions, and follows specific standards.
Joghataiee et al. [21] emphasized the multidimensionality of the education process, highlighting the importance of modern educational methods. Larijani et al. [22] considered skill training in the rehabilitation education process to be based on problem-solving skills, individual participation, and group interactions. They also suggested that the use of virtual education methods and the use of new technologies and effective educational tools to be very important in rehabilitation education. Zehry et al. [23] considered e-learning and the use of educational tools as effective facilitators of the learning process. Karimi et al. [24] believed that improved learning outcomes is based on optimal interpersonal communication. Seyedi et al. [25], by emphasizing the effectiveness of blended learning, suggested e-learning as a key factor in enhancing educational outcomes. Masoumi et al. [26] reported that the use of a conceptual model based on the components of education that includes the subject matter, course, and lesson, can effectively improve learning motivation. Hosseini et al. [27] highlighted the role of teaching methods in improving learning motivation and increasing educational productivity. Gholami et al. [28] identified teamwork as an effective factor in enhancing motivation and achieving improved educational outcomes. Assaf et al. [29] highlighted the role of creating active learning opportunities in the learners’ progress, and Toothake and Taliaferro [30] emphasized continuity and consistency as influential factors in effective learning. Trabulsi [31] identified students’ interest in the subject matter and their positive attitudes as key elements of successful rehabilitation education. Stock-Schröer et al. [32] further demonstrated that coordinated instruction and the development of a coherent and comprehensive curriculum contribute significantly to effective rehabilitation education. Zare Bidaki et al. [33] emphasizesd the role of digital technologies and multimedia in improving learning outcomes. Gibson et al. argued that rehabilitation education is distinguished from other educational fields by the unique nature of rehabilitation disciplines, which is rooted in underlying philosophies of empowerment. Accordingly, to improve the rehabilitation education process, they underscored the importance of a coherent curriculum, a right attitude toward rehabilitation medicine, and the standardization of rehabilitation medicine education [34]. Chung found that community-based learning enhance the learning process by strengthening problem-solving abilities, promoting critical thinking, and improving active learning among learners [35]. Battista et al. identified arts-based skills, practical instruction, and teamwork as effective facilitators of learning in rehabilitation education [36]. Overall, rehabilitation education is most effective when educational processes and methods are aligned with the fundamental principles and philosophy of rehabilitation.
There were some limitations in the study. The interviews were time-consuming which may affect the responses. There was a scant research on rehabilitation education in Iran, to compare the results; to address this limitation, additional searches were conducted for related articles in English language. The samples were recruited only from the University of Social Welfare and Rehabilitation Sciences, which may limit the generalizability of the findings. To enhance the generalizability, feedback and confirmatory perspectives were obtained from faculty members at other rehabilitation universities in Iran.
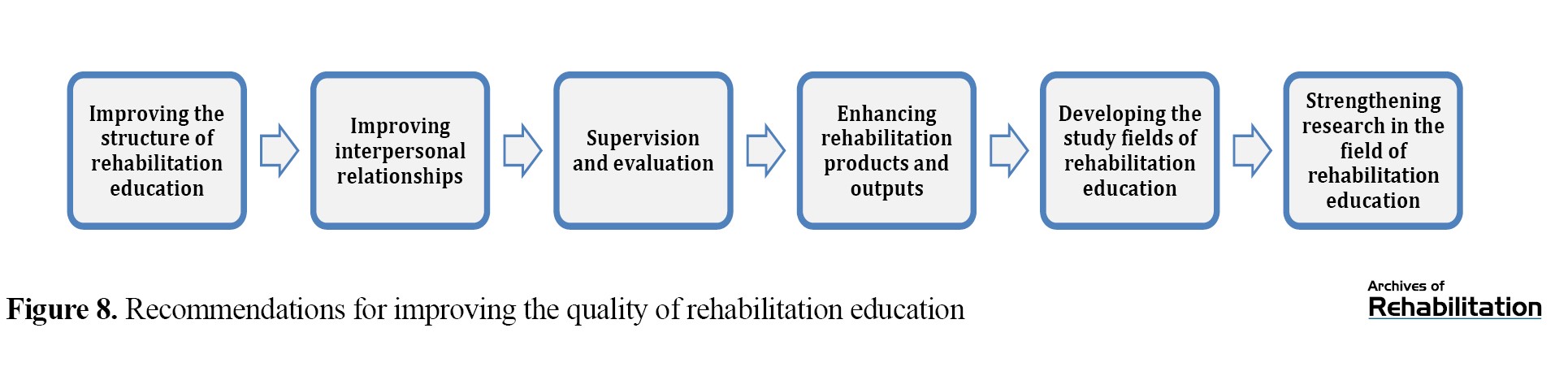
Recommendations derived from the study for improving rehabilitation education were organized into six categories (Table 8).
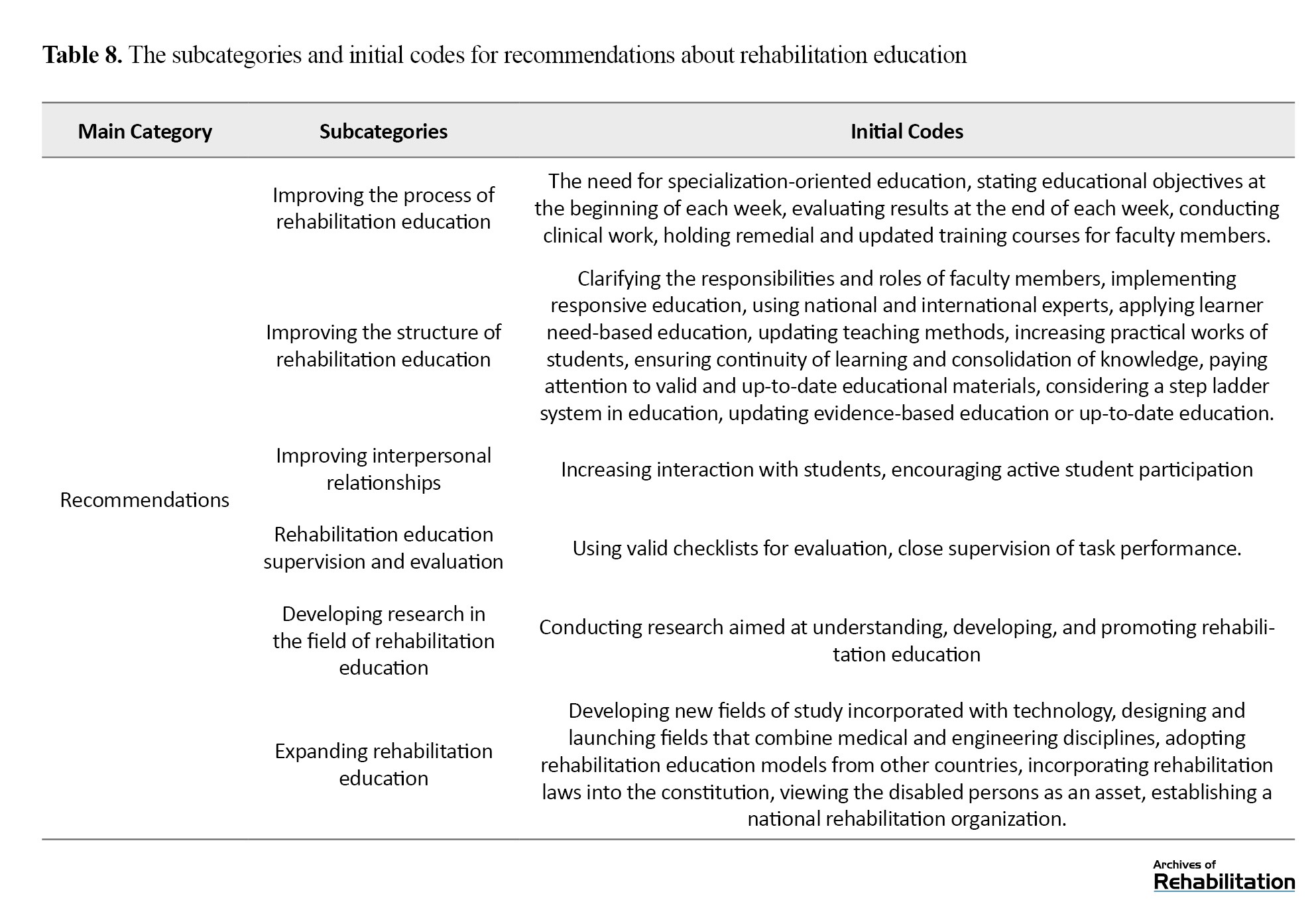
These categories focus on improving the rehabilitation education process, structure, monitoring and evaluation, and strengthening research in the field of rehabilitation education in Iran and the expansion of rehabilitation education.
Figure 8 plots the diagram of recommendations derived from the mentioned six categories.
There were some limitations in the study. The interviews were time-consuming which may affect the responses. There was a scant research on rehabilitation education in Iran, to compare the results; to address this limitation, additional searches were conducted for related articles in English language. The samples were recruited only from the University of Social Welfare and Rehabilitation Sciences, which may limit the generalizability of the findings. To enhance the generalizability, feedback and confirmatory perspectives were obtained from faculty members at other rehabilitation universities in Iran.
Recommendations derived from the study for improving rehabilitation education were organized into six categories (Table 8).
These categories focus on improving the rehabilitation education process, structure, monitoring and evaluation, and strengthening research in the field of rehabilitation education in Iran and the expansion of rehabilitation education.
Figure 8 plots the diagram of recommendations derived from the mentioned six categories.
Each of the concepts mentioned in these categories encompasses micro, macro, and meso policies of rehabilitation education and provides the possibility of improving rehabilitation education equality.
Conclusion
For optimal rehabilitation education, active learning methods, practical training, teamwork, collaborative learning, coordinated teaching, skill training, a conceptual map of education, focusing on education strategies, and a coherent curriculum are important. Improvement in the learning process is closely related to learners’ motivation and interest, which is affected by effective communication among educational stakeholders and learners’ positive attitudes toward rehabilitation. Educational tools, particularly digital technologies, play an important role in enhancing rehabilitation education, and blended and multidimensional learning is an effective factor in improving rehabilitation education. The main constructs shaping the nature of rehabilitation education are focused on the centrality of the client, the multidimensionality of education, and the need for teamwork dependent on cultural and local contexts.
In conclusion, the implementation of proper rehabilitation education in Iran requires attention to the multiple dimensions and determinants of the education program, the specific characteristics of rehabilitation education, the use of correct and appropriate methods and tools for rehabilitation education, attention and focus on the process and products of rehabilitation education, the correct selection of students and their appropriate training, interdisciplinary interactions, the use of effective study fields, and the motivation of learners. Practical recommendations for improving rehabilitation education include:
1) defining the structure of rehabilitation education and devoting a branch of higher education to rehabilitation education. 2) developing detailed educational protocols for rehabilitation work with people in need of these services. 3) focusing on the components of rehabilitation education and developing comprehensive and equity-oriented rehabilitation programs. 4) utilizing modern rehabilitation teaching methods. 5) applying the novel education methods for improving learning motivation. 6) new planning and policymaking focused on addressing the problems of rehabilitation education. 7) improving rehabilitation skill training during the education process. 8) applying the specific requirements of rehabilitation education in the teaching process.
Ethical Considerations
Compliance with ethical guidelines
All interviews in this study were conducted after obtaining informed consent from the participants. The confidentiality of their information was observed. An ethical approval code was obtained from the University of Social Welfare and Rehabilitation Sciences (Code: IR. USWR.REC.1395.331).
Funding
This study was funded by the University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Conceptualization, editing and review: Ghoncheh Raheb and Nahid Rahmani; investigation and data collection: All authors.
Conflict of interest
The authors declared no conflict of interest.
Conclusion
For optimal rehabilitation education, active learning methods, practical training, teamwork, collaborative learning, coordinated teaching, skill training, a conceptual map of education, focusing on education strategies, and a coherent curriculum are important. Improvement in the learning process is closely related to learners’ motivation and interest, which is affected by effective communication among educational stakeholders and learners’ positive attitudes toward rehabilitation. Educational tools, particularly digital technologies, play an important role in enhancing rehabilitation education, and blended and multidimensional learning is an effective factor in improving rehabilitation education. The main constructs shaping the nature of rehabilitation education are focused on the centrality of the client, the multidimensionality of education, and the need for teamwork dependent on cultural and local contexts.
In conclusion, the implementation of proper rehabilitation education in Iran requires attention to the multiple dimensions and determinants of the education program, the specific characteristics of rehabilitation education, the use of correct and appropriate methods and tools for rehabilitation education, attention and focus on the process and products of rehabilitation education, the correct selection of students and their appropriate training, interdisciplinary interactions, the use of effective study fields, and the motivation of learners. Practical recommendations for improving rehabilitation education include:
1) defining the structure of rehabilitation education and devoting a branch of higher education to rehabilitation education. 2) developing detailed educational protocols for rehabilitation work with people in need of these services. 3) focusing on the components of rehabilitation education and developing comprehensive and equity-oriented rehabilitation programs. 4) utilizing modern rehabilitation teaching methods. 5) applying the novel education methods for improving learning motivation. 6) new planning and policymaking focused on addressing the problems of rehabilitation education. 7) improving rehabilitation skill training during the education process. 8) applying the specific requirements of rehabilitation education in the teaching process.
Ethical Considerations
Compliance with ethical guidelines
All interviews in this study were conducted after obtaining informed consent from the participants. The confidentiality of their information was observed. An ethical approval code was obtained from the University of Social Welfare and Rehabilitation Sciences (Code: IR. USWR.REC.1395.331).
Funding
This study was funded by the University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Conceptualization, editing and review: Ghoncheh Raheb and Nahid Rahmani; investigation and data collection: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Talebi A, Nourbakhsh N, Mottaghi P, Dadgostarnia M, Vafamehr V. [New teaching/learning model for medical students, according to integration of usual educational methods in Isfahan University Of Medical Sciences (Persian)]. Iranian Journal of Medical Education. 2011; 10(5):1198-208. [Link]
- Vameghi M, Jorjoran Shushtari Z, Takaffoli M, Bahrami G, Setareh Forouzan A. [Investigating the requirements for integration of the social determinants of health approach in rehabilitation education: A qualitative study in Iran (Persian)]. Archives of Rehabilitation. 2024; 25(S3):576-603. [DOI:10.32598/RJ.25.specialissue.2573.2]
- Patterson A, Lohman H, Bahle-Lampe A, Mu K, Greiner B, Qi Y, et al. Meeting global rehabilitation needs: The development and evaluation of an international visiting rehabilitation student program. Journal of Allied Health. 2020; 49(2):99-105. [Link]
- Rastegar T, Hoshyari Manesh S, Salari H. [Effect of team based learning on rehabilitation students anatomy learning (Persian)]. Journal of Ilam University of Medical Sciences. 2016; 23(6):163-8. [Link]
- Hamidi. [Education and research is a process of planning, assessing, processing, and writing (Persian)]. Tehran: Sogand Publication; 2006. [Link]
- Borhan E, Azimi K, Shahrabi. [Applying correlation rules and cluster analysis in pathology and academic failure of students at Sharif University of Technology (Persian)]. Paper presented at: 1st Iran Data Mining Conference. 2007 November 17; Tehran, Iran. [Link]
- Ferasatkhah M. [The future view of Iranian higher education quality; a grounded theory based model (Persian)]. Journal of Research and Planning in Higher Education . 2004; 14(4):67-95. [Link]
- Raheb G, Khani A, Jandaghi J, Sabzi Khoshnami M. Evaluating the Level of Learning Motivation Among the Rehabilitation Students at the University of Social Welfare and Rehabilitation Sciences of Tehran, Iran; During 2011-2012. Middle East Journal of Rehabilitation and Health Studies. 2014; 1(2):e23611. [DOI:10.17795/mejrh-23611]
- Turoff M. An end to student segregation: No more separation between distance learning and regular courses. On the Horizon. 2000; 8(1):1-7. [DOI:10.1108/10748120010803294]
- Mardani Givi M, Asadi K, Haghighi M, Saheb Ekhtiari K, Hashemi Motlagh K. [Evaluation of references' accuracy and their influential factors in medical and dental dissertations of Guilan University of Medical Sciences between 2006 and 2011 (Persian)]. Research in Medical Education. 2011; 3(2):19-28. [Link]
- Chen S. A cognitive model for non-linear learning in hypermedia programmes. British Journal of Educational Technology. 2002; 33(4):449-60. [DOI:10.1111/1467-8535.00281]
- Carbonaro M, King S, Taylor E, Satzinger F, Snart F, Drummond J. Integration of e-learning technologies in an interprofessional health science course. Medical Teacher. 2008; 30(1):25-33. [DOI:10.1080/01421590701753450] [PMID]
- Ford N, Wood F, Walsh C. Cognitive styles and searching. Online and CD-Rom Review. 1994; 18(2):79-86. [DOI:10.1108/eb024480]
- Negrini S, Selb M, Kiekens C, Todhunter-Brown A, Arienti C, Stucki G, et al. Rehabilitation definition for research purposes. A global stakeholders’ initiative by Cochrane Rehabilitation. Neurorehabilitation and Neural Repair. 2022; 36(7):405-14. [DOI:10.1177/15459683221093587] [PMID]
- Rahmani N, Kajbafvala M, Takian A, Shirazikhah M, Hamidi H, Ehsanzadeh SJ. A comparative study of rehabilitation policies in selected countries: A narrative review. Archives of Rehabilitation. 2024; 25(1):2-25. [DOI:10.32598/RJ.25.1.1282.3]
- Moradi F, Kazemi-Karyani A, Karamimatin B, Soltani P, Kamali M, Jalili F, et al. [Socioeconomic disparities in the prevalence of disability in iran: A decomposition analysis using the concentration index (Persian)]. Archives of Rehabilitation. 2025; 26(2):166-87. [DOI:10.32598/RJ.26.2.1719.1]
- Karimidermani H. [Rehabilitation of special groups with emphasis on social work services (Persian)]. Tehran: Roshd; 2011. [Link]
- Seif AA. [Educational Psychology (Persian)]. Tehran: Agah Publication. 2012. [Link]
- Raheb G, Hamidi MA, Akhavan Tafti M, Rezabakhsh H. [Designing and testing an educational model to improve learning motivation based on social constructivist thinking (Persian)]. Journal of Behavioral Science. 2008; 3(1)79-83. [Link]
- Witek D, Dalgin RS. Collaborative information literacy practices to connect theory to practice in rehabilitation counseling students. Collaborative Librarianship. 2019; 11(3):6. [Link]
- Joghataiee M, ShiraziM , Taavoni S. [Studying the Use of Modern Teaching Methods by Professors of the Faculty of Pharmacy, International Campus, Tehran University of Medical Sciences in 2011-2012-2014 (Persian)]. Paper presented at: The First National Conference on Teaching and Learning Methods in The Field and University. 20 May 2014; North Khorasan, Iran.
- Larijani B, Motevaseli E. [New methods of teaching medical ethics (Persian)]. Iranian Journal of Diabetes and Metabolism. 2004; 4:39-46. [Link]
- Meinel FG, Dimitriadis K, von der Borch P, Störmann S, Niedermaier S, Fischer MR. More mentoring needed? A cross-sectional study of mentoring programs for medical students in Germany. BMC Med Educ. 2011; 11(68). [DOI:10.1186/1472-6920-11-68]
- Karimi Moanaghi H, Rad M, Bakhshi M. [Do modern teaching methods have the necessary effectiveness in medical education in Iran?: A systematic review (Persian)]. Strides in Development of Medical Education. 2013; 10(2):153. [Link]
- Seyedi M, Yaghoubi Z. [Designing and implementing a blended learning system for training students in rehabilitation fields (Persian)]. 2014; 3(2):42-50. [Link]
- Masoumi M, Ebadi A, Daneshmandi M, Raeisifar A. Concept mapping modern teaching strategy in nursing education. Education Strategies in Medical Sciences. 2011; 4(1):47-51. [Link]
- Hosseini M, Ahmadieh MH, Shavazi MA, Farsani SE. Study skills in bachelor students in the School of Public Health, Yazd, 2006. Strides in Development of Medical Education. 2008; 5(2):88-93. [Link]
- Gholami T, Kouhpayeh SA, Ramezani M, Mobasheri F. Public health students’ attitudes toward team-based learning method in Fasa University of Medical Sciences. Educational Development of Judishapur. 2018; 9(1):30-7. [Link]
- Assaf MM, Al-Jamal DA, Rababeh EQ. The effect of an electronic collocation-based instructional program on enhancing Jordanian EFL tenth grade students’ reading comprehension. IUG Journal of Educational & Psychological Studies. 2020; 28(4). [Link]
- Toothaker R, Taliaferro D. A phenomenological study of millennial students and traditional pedagogies. Journal of Professional Nursing. 2017; 33(5):345-9. [DOI:10.1016/j.profnurs.2017.01.004] [PMID]
- Trabulsi RU. Accounting students’attitudes toward traditional and modern teaching methods: the saudi context. Academy of Accounting and Financial Studies Journal. 2018; 22(5):1-6. [Link]
- Stock-Schröer B, Huber R, Joos S, Klose P. Evaluation of the current status of Rehabilitation, Physical Medicine and Naturopathy education 10 years after the reform of the Medical Licensure Act-a nationwide survey of German Medical Universities. GMS Journal for Medical Education. 2017; 34(1): Doc3. [Link]
- Zare Bidaki M, Yousefi M, Malaki Moghadam H, Rajabpour Sanati A, Nazari-Alam A. [The effectiveness of clip-based education on academic learning and satisfaction in microbiology course of health students (Persian)]. Journal of Translational Medical Research. 2018; 25(S):37-45. [Link]
- Gibson J, Lin X, Clarke K, Fish H, Phillips M. Teaching medical students rehabilitation medicine. Disability and Rehabilitation. 2010; 32(23):1948-54. [DOI:10.3109/09638281003797364] [PMID]
- Chung EY-h. Facilitating learning of community-based rehabilitation through problem-based learning in higher education. BMC medical education. 2019; 19(1):433. [DOI:10.1186/s12909-019-1868-4] [PMID]
- Battista S, Furri L, Pellegrini V, Giardulli B, Coppola I, Testa M, et al. Which lecturers’ characteristics facilitate the learning process? A qualitative study on students’ perceptions in the rehabilitation sciences. BMC Medical Education. 2023; 23(1):431. [DOI:10.1186/s12909-023-04308-y] [PMID]
Type of Study: Original |
Subject:
Rehabilitation Management
Received: 14/07/2025 | Accepted: 3/12/2025 | Published: 1/01/2026
Received: 14/07/2025 | Accepted: 3/12/2025 | Published: 1/01/2026
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
