

Volume 26, Issue 2 (7-2025)
Arch Rehabil 2025, 26(2): 278-295 |
Back to browse issues page


Ethics code: IR.USWR.REC.1402.082
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Seyedi S, Abdi K, Basakha M, Hosseinzadeh S. Examining the Translation and Validation of the Persian Version of Assistive Technology Device Predisposition Assessment in Adults With Disabilities. Arch Rehabil 2025; 26 (2) :278-295
URL: http://rehabilitationj.uswr.ac.ir/article-1-3576-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3576-en.html

1- Department of Rehabilitation Management, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Rehabilitation Management, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. & Social Determinants of Health Research Center, Social Health Research Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,k55abdi@yahoo.com
3- Social Determinants of Health Research Center, Social Health Research Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. & Department of Social Welfare Management, School of Social Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Rehabilitation Management, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. & Social Determinants of Health Research Center, Social Health Research Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
3- Social Determinants of Health Research Center, Social Health Research Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. & Department of Social Welfare Management, School of Social Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
Keywords: People with disabilities, Assistive technology, Validation, Usability assessment, Validity and reliability
Full-Text [PDF 1952 kb]
(1146 Downloads)
| Abstract (HTML) (4623 Views)
Full-Text: (869 Views)
Introduction
Assistive technologies encompass a range of tools and services designed to support people with chronic conditions, disabilities, elderly individuals, and those facing temporary or permanent impairments [1]. Through a variety of tools and services, these technologies enhance independence and social participation for these groups. Examples of assistive technologies include wheelchairs, hearing aids, white canes, text-to-speech software, and medication organizers [2].
According to a report by the World Health Organization (WHO), 15% of the global population lives with a disability [3]. Additionally, approximately 2.5 billion people rely on assistive technologies to lead a better and more independent life. This number is expected to rise to 3.5 billion by 2050 due to an aging population and the increasing prevalence of non-communicable diseases [4]. Given Iran’s estimated population of around 91.5 million in 2024 [5], an estimated 13.7 million people in the country will experience a disability.
Hence, ensuring access to accessible, appropriate, and affordable assistive technologies is a fundamental human right and a public health and development priority [6]. Moreover, bridging existing gaps is crucial for achieving the sustainable development goals and ensuring the effective implementation of the convention on the rights of persons with disabilities [3].
Despite the widespread need for and positive impact of assistive technologies, access remains significantly limited. Evidence suggests that 90% of individuals in need of assistive technologies are unable to obtain them [3]. However, if the provision of these technologies does not take users’ needs and preferences into account, they may fail to deliver a satisfactory experience. This mismatch can lead to improper use or even abandonment of these technologies [7]. Therefore, aligning assistive technologies with users’ needs and preferences is crucial for their adoption and effectiveness [8].
Various assessment tools have been developed to evaluate user satisfaction and the impact of assistive technologies on functional outcomes, facilitating decision-making and monitoring their use [9]. These tools help improve product design, advance scientific research, shape public policies, and emphasize the importance of assistive technologies in sustaining rehabilitation programs [9, 10].
Despite the critical need for standardized assessment tools, Iran lacks a reliable method for evaluating how well assistive technologies meet the needs of individuals with disabilities. Although the rapid assistive technology assessment tool has been translated into Persian and its face validity has been established, its primary purpose is to assess the prevalence of assistive technology use and needs in the population [11]. This study aims to translate and adapt the consumer form of the ATD-PA and to assess its validity and reliability for adults with disabilities in Iran.
Materials and Methods
This study employed a methodological research design and was conducted in 2023–2024. The target population included adults with disabilities receiving support from the Welfare Organization of Ardabil Province, Iran, and using assistive technology devices. Non-probability quota sampling was employed.
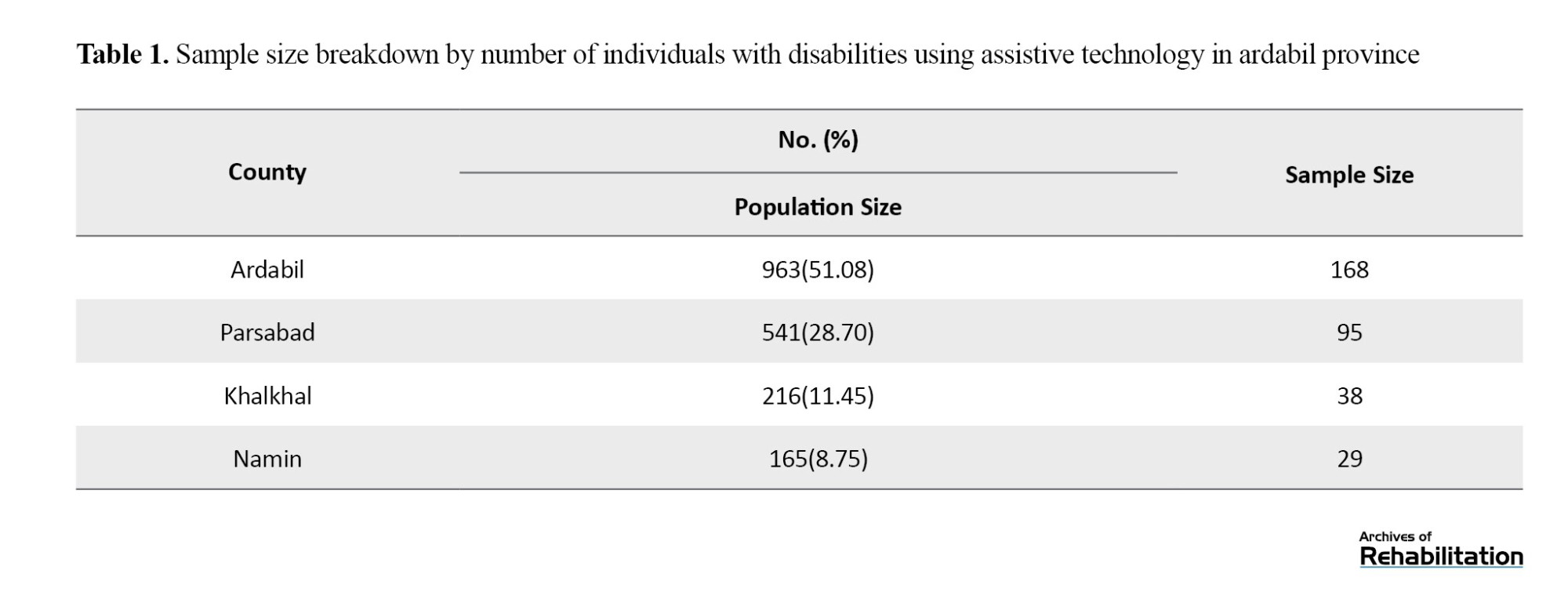
To ensure proper representation, coordination was made with the General Directorate of the Welfare Organization of Ardabil Province, Iran, and the study population was categorized according to the number of assistive technology users in four counties of Ardabil Province (cities of Ardabil, Parsabad, Khalkhal, and Namin). The sample distribution for each county is presented in Table 1.
Inclusion and exclusion criteria
The inclusion criteria were as follows: the individual must have a disability classified as severe or very severe by the Welfare Organization’s medical-rehabilitation commission and be receiving support from the Welfare Organization in Ardabil Province, Iran. Additionally, the individual must be over 18 years old, willing to participate in the research, and able to communicate in Persian. Meanwhile, the individual must also have used at least one assistive technology in the past two months. Subsequently, the exclusion criterion was incomplete questionnaire responses.
Study instruments
In this study, the Assistive Technology Device Predisposition Assessment (ATD PA) was used. Designed by Marcia J. Scher in 1996, this tool assesses the best match between an individual and assistive technology for people over 18 years old [12]. It is part of the matching person and technology (MPT) model, which examines the individual’s characteristics, environment, and technology. The MPT model is based on the International Classification of Functioning, Disability, and Health (ICF) framework, and its goal is to provide a comprehensive evaluation of users’ goals, preferences, environmental factors, and assistive technology [12].
The ATD-PA consists of two forms: one for consumers (users) and one for professionals. The consumer form contains four sections. The first section evaluates individuals’ performance across nine functional domains, including thinking, decision-making and remembering, seeing, hearing, speaking and communicating, muscle power and physical endurance, control of arms, shoulders, trunk, grasping and control of fingers, control of hips, legs, feet, and control of voluntary movement. This section uses a 5-point Likert scale to score responses. The second section evaluates activities, participation, and quality of life through 12 questions, with the average score representing overall quality of life. The third section assesses psychological, social, and emotional characteristics using 32 statements, which are scored accordingly. The fourth section, known as the device form, evaluates consumers’ expectations of the assistive technology they use, based on 12 questions. This tool helps create a consumer profile, enabling rehabilitation professionals to identify functional areas that need intervention [12].
In assessing the internal consistency of the quality-of-life subscale (Section B) of the original ATD-PA version, a Cronbach α of 0.80 indicated good reliability [8]. In studies conducted by the author in 2005 and 2010, the ATD-PA’s high internal consistency and predictive validity were confirmed [13, 14]. Furthermore, a strong correlation between the ATD-PA and the life satisfaction scale was found (Spearman’s Ρ=0.89) [14].
Implementation method
Permission to use the tool was initially obtained from the questionnaire’s designer. The translation process followed the forward-backward method, adhering to the WHO’s recommended standards [15]. First, the tool was translated from English into Persian by a bilingual translator. Next, a back-translation into English was performed by another bilingual translator, who had no previous knowledge of the original. This ensured the accurate conveyance of core concepts and content. The two versions were reviewed in collaboration with rehabilitation and assistive technology experts, incorporating their feedback to finalize the translation. The newly translated English version was then sent to the original author of the questionnaire for review. After receiving approval for conceptual equivalence and consistency with the original, the final Persian version was reviewed by rehabilitation specialists and individuals with disabilities to assess face and content validity.
Two indices, namely content validity ratio (CVR) and content validity index (CVI), were used for quantitative content validity assessment. After collecting the survey questionnaires, expert feedback was analyzed statistically based on CVR and CVI values, resulting in modifications, such as item removal, addition, or revision. The Lawshe method was used to calculate the CVR and determine content validity [16]. Fifteen rehabilitation specialists evaluated the Persian version, rating each item as “essential,” “useful but not essential,” or “not necessary.” Experts also assessed each item’s clarity and relevance. Items with a CVR<0.49 were eliminated. For CVI assessment, specialists evaluated each item for clarity, simplicity, and relevance according to Waltz and Bausell’s guidelines [17]. The percentage of experts selecting the top two categories was then calculated. Items scoring <0.70 were rejected, those between 0.70 and 0.79 required revision, and those >0.79 were deemed acceptable.
Face validity was assessed by collecting feedback from 6 experts and individuals with disabilities on the comprehensibility of the tool’s questions. Revisions were made based on their suggestions.
Factor analysis was conducted to assess the construct validity of the ATD-PA tool. Sample size was determined based on scientific recommendations, suggesting 5 to 10 participants per item [18] and a minimum of 200 participants for factor analysis [19]. Given the 66 items in the tool, a sample of 330 participants was selected for the construct validity assessment. Data adequacy for factor analysis was assessed using the Kaiser-Meyer-Olkin index and the Bartlett test. The varimax rotation method was used to facilitate factor interpretation [20]. The purpose of these analyses was to identify the underlying factors within the items.
The tool’s reliability was assessed through internal consistency and test-retest reliability measures. Due to structural differences among the four sections and the absence of a definitive theoretical model for each, confirmatory factor analysis was not conducted for the ATD-PA tool. Internal consistency was assessed using the Cronbach α coefficient.
Following approval from the Ardabil Welfare Organization and participant selection based on eligibility criteria from the Armaghan system, participant conditions were confirmed via phone calls. Informed consent was then obtained from individuals with disabilities for study participation. Participants attended welfare centers in various counties, where the researcher provided detailed instructions on completing the questionnaire. The participants then completed the ATD-PA tool.
In the final stage, test-retest reliability was assessed by having 30 individuals with disabilities complete the questionnaire again after two weeks. The intraclass correlation coefficient (ICC) was then calculated with a 95% confidence interval (CI).
Statistical analysis
Descriptive statistics were used to summarize participant characteristics, and data analysis, including factor analysis, was performed using SPSS software, version 23.
Results
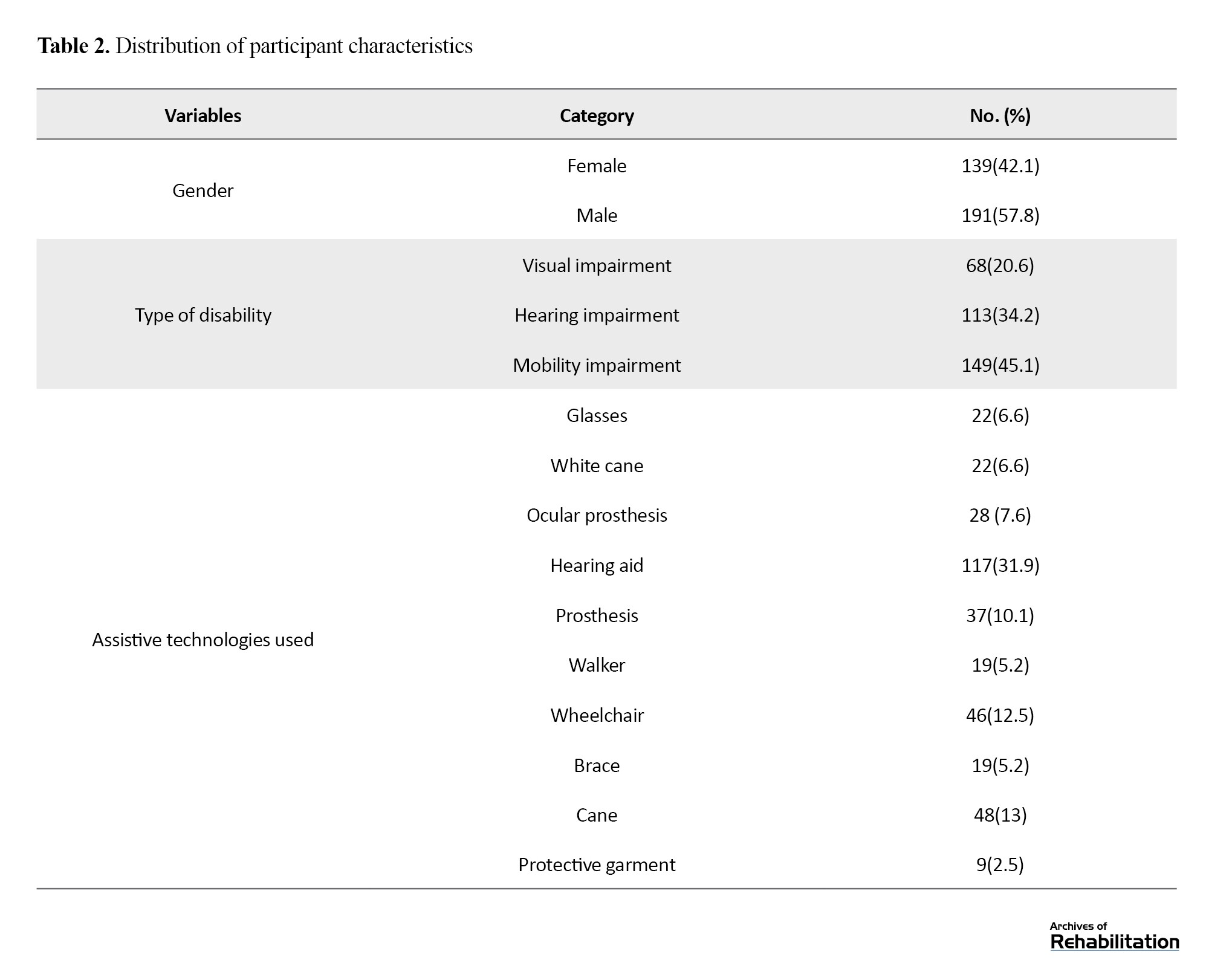
A total of 330 individuals participated in this study, 57.8% of whom were male. The participants’ Mean±SD age was 43±12.61 years . The largest age group was 31–40 years, representing 25.5% of the participants. Additionally, 45.1% of participants had mobility impairments, and 11.21% used more than two assistive technology devices. The distribution of participant characteristics is presented in Table 2.
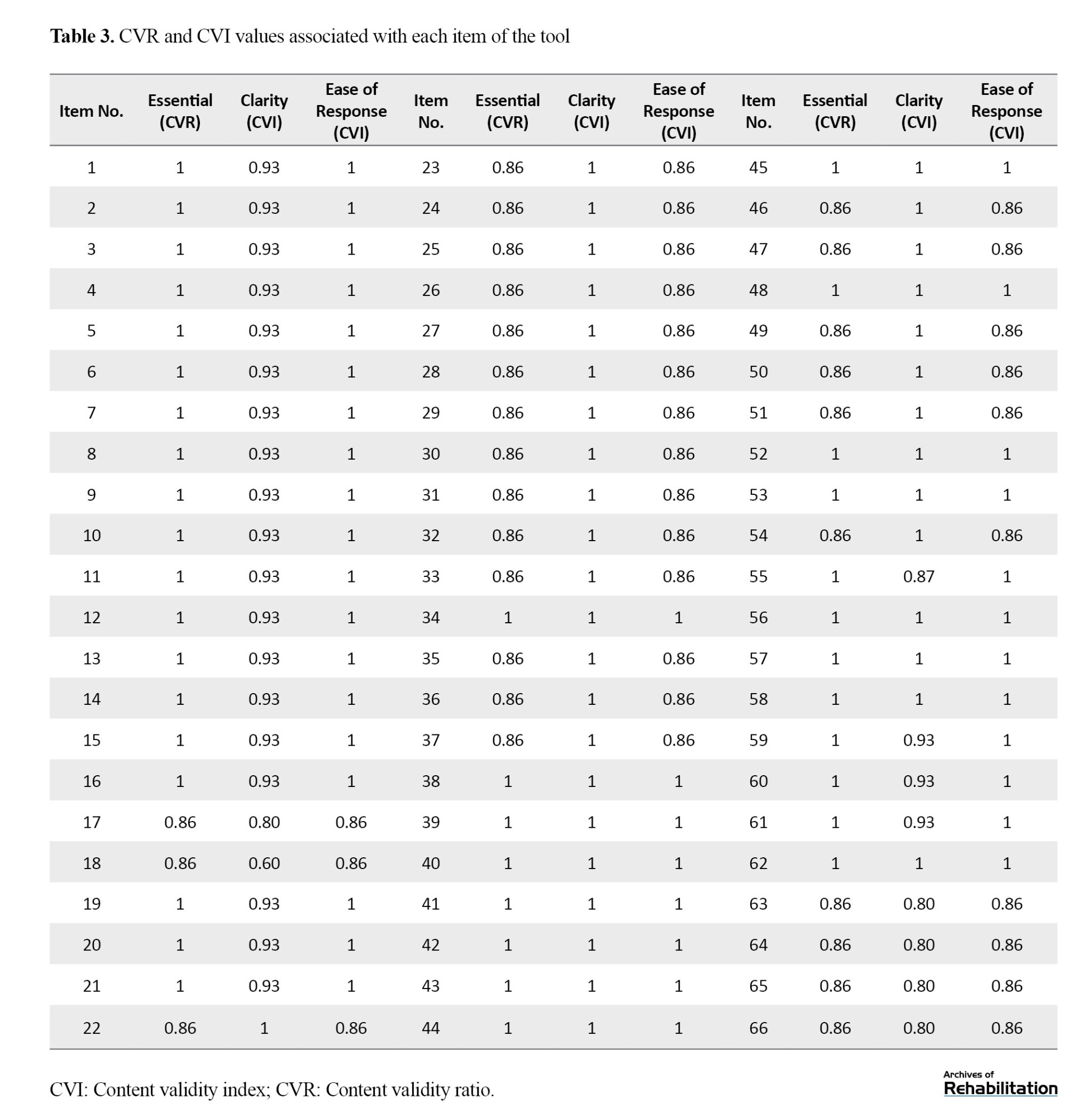
In Table 3, the CVR and CVI for the ATD-PA tool were calculated and analyzed. The results indicated that CVR=0.94 and CVI=0.95, both demonstrating a very high level of content validity for this assessment tool.
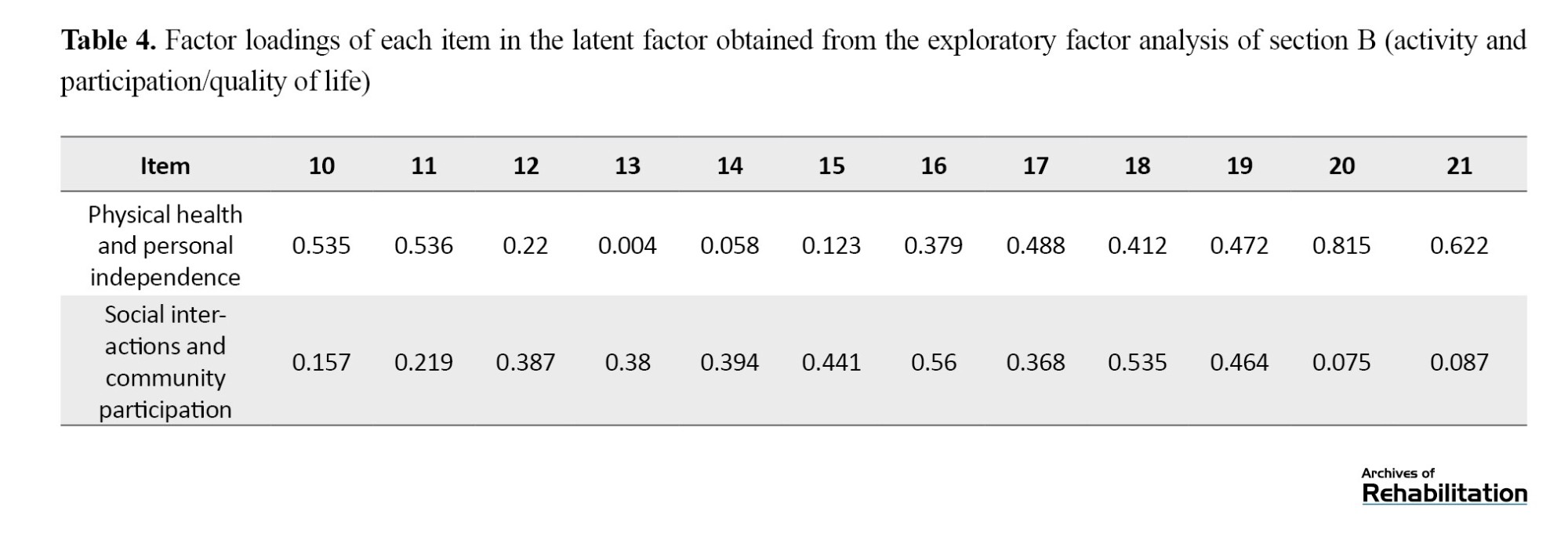
Exploratory factor analysis for Section B (activity and participation or quality of life) of the questionnaire, consisting of 12 items, was conducted using the maximum likelihood method with varimax rotation. The analysis identified two latent factors: physical health and personal independence, and social interactions and community participation. The Kaiser-Meyer-Olkin measure for this section was 0.884, indicating adequate data for factor analysis. Additionally, the Bartlett test (χ²=973.03, P<0.001) confirmed significant correlations among the items. Based on these findings, the two identified factors accounted for 34.5% of the total variance, with Factor 1 explaining 20.3% and Factor 2 explaining 14.2%. The item loadings for each factor are presented in Table 4.
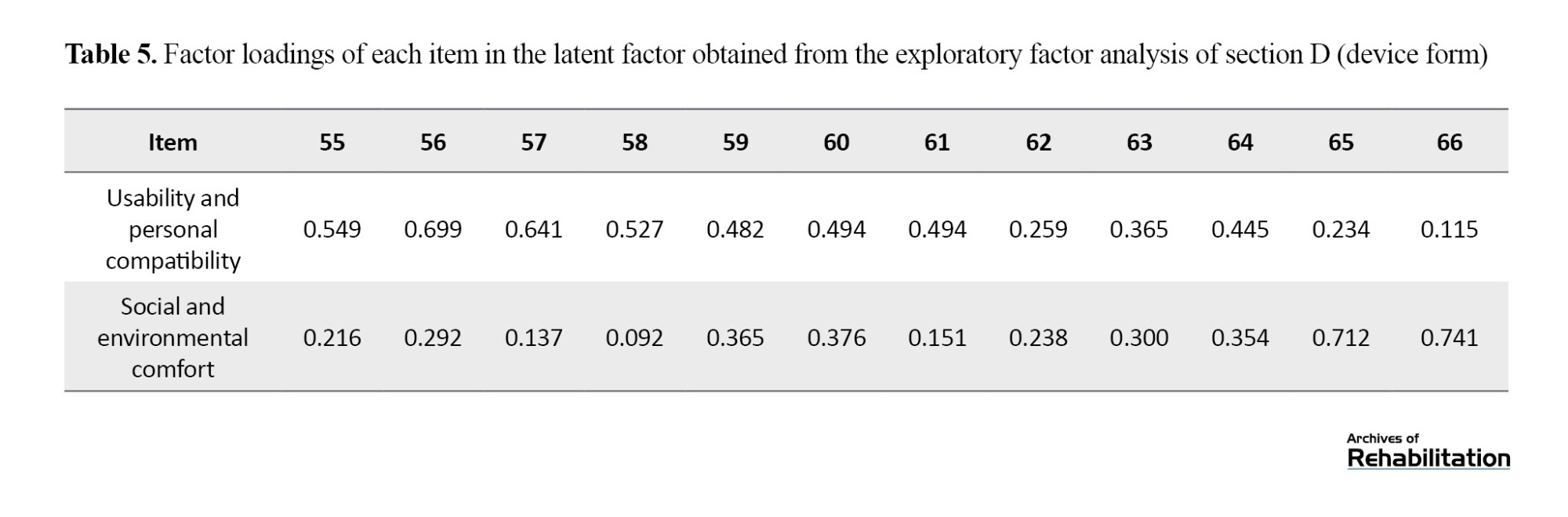
Exploratory factor analysis for Section D (device form) of the questionnaire, consisting of 12 items, was performed using the maximum likelihood method with varimax rotation. The analysis identified two latent factors: usability and personal compatibility, and social and environmental comfort. The Kaiser-Meyer-Olkin value for this section was 0.865, indicating the adequacy of the data for factor analysis. Additionally, Bartlett’s test (χ²=1066.96, P<0.001) showed significant correlations among the items. Based on the results, the two identified factors explained 37.1% of the total variance in the scores, with the first factor explaining 22.3% and the second factor explaining 14.8%. The items for each factor and their factor loadings are presented in Table 5.
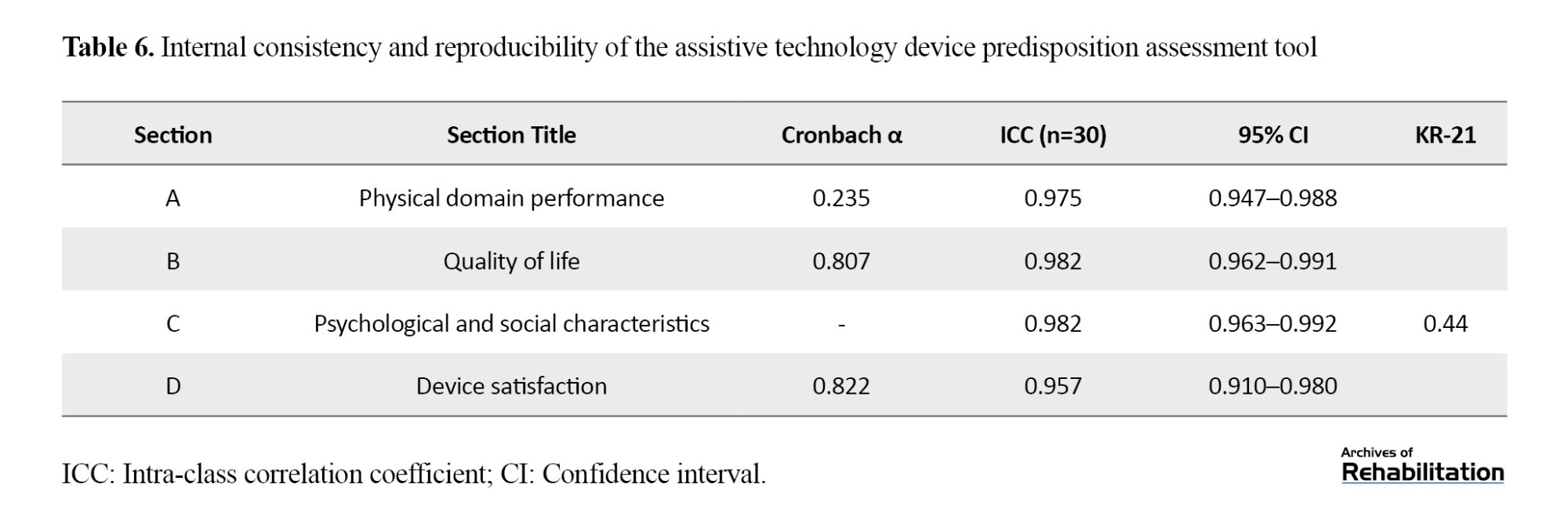
The reliability results of the test, including the intraclass ICCs and the Cronbach α values, are shown in Table 6.
Discussion
To develop the Persian version of the ATD-PA scale, a multi-step process was followed, including initial translation, version unification, and back-translation into the original language. The final version was refined through multiple review sessions by the research team, followed by assessments of face validity, content validity, and construct validity.
In the face validity assessment, no items were eliminated. However, based on expert feedback, modifications were made to items 41 and 63 to 66. Content validity was confirmed with a CVR of 0.94 and a CVI of 0.95, demonstrating the accuracy and precision of the questions in measuring the intended characteristics. These findings align with international studies. In Brazil, the conceptual, semantic, and operational adaptation of the ATD-PA tool was validated with high expert agreement [21]. Similarly, in Germany, strong content validity for this tool was reported, highlighting its reliability in evaluating assistive technologies [22].
Regarding construct validity, the study revealed that while some underlying factors were identified, the explained variance for Sections B (activity and participation or quality of life) and D (device form) was below 50%, indicating the need for revision in these sections. Some of our findings contrast with international studies. For instance, a study in Greece reported satisfactory construct validity for subscales such as adaptability, usability, and satisfaction with assistive technology [23]. Additionally, in this study, Section A (performance) showed a low Cronbach α of 0.235, and Section C (psychosocial characteristics) had a KR-21 value of 0.447, indicating weak reliability. As a result, factor analysis was not conducted for these sections.
In the test, re-test reliability assessment, the ICC values for all sections, measured over a two-week interval, were notably high, ranging from 0.957 to 0.982. These results reflect strong agreement and reliability across all sections, which is consistent with international studies, such as those in Greece (ICC=0.981) and Italy (ICC=0.981) [23, 24].
The obtained Cronbach α values for Section B (0.807) and Section D (0.822) indicate good internal consistency, which aligns with reports from Italy (α=0.702–0.804) [24] and the United States (α=0.80) [13]. These results also correspond with findings from Alves et al. in Brazil, who reported moderate to excellent reliability for the ATD-PA tool [21]. However, the low Cronbach α for Section A (0.235) suggests that the structure of the questions assesses different dimensions within each section. Although the Cronbach α for Section C was not reported, its high ICC (0.982) indicates strong agreement.
The availability of appropriate tools for evaluating the compatibility of assistive technologies with users can have a positive impact on their lives, fostering technological advancements and improving service delivery [25]. These tools not only assess user satisfaction and functional improvements but also measure the impact of assistive technology use over a specified period [9].
The ATD-PA tool has been used in previous research to evaluate the capabilities of assistive technologies across various populations, demonstrating its scientific validity [12].
Conclusion
The Persian version of the ATD-PA demonstrates acceptable psychometric properties for evaluating the experiences of individuals using assistive technologies. Therefore, like the original version, the Persian adaptation is a reliable and valid tool suitable for both clinical and research settings.
Study limitations
Due to the large number of items in this scale and the time required for completion, some rehabilitation service providers, including the Welfare Organization, faced time and resource constraints. These challenges may hinder the creation of comprehensive user profiles, potentially impacting the accuracy and efficiency of assessments. Additionally, reliance on self-reporting by users could reduce evaluation accuracy, as some participants may find it difficult to fully articulate their experiences.
Ethical Considerations
Compliance with ethical guidelines
Informed consent was obtained from participants or their legal guardians. Ethical principles were strictly adhered to, ensuring confidentiality and privacy. Participation was entirely voluntary, and individuals could withdraw from the study at any stage without consequences. This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1402.082).
Funding
This article is derived from Soheila Seyedi’s master’s thesis, which was approved by the Rehabilitation Management Department at the University of Social Welfare and Rehabilitation Sciences. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Methodology, validation, analysis, editing, and finalization, conceptualization, investigation, literature Review, and Manuscript Drafting: All authors; Visualization, supervision, and project management: Kianoush Abdi; Funding Acquisition: Soheila Seyedi.
Conflict of interest
The authors declare no conflicts of interest.
Acknowledgments
The authors extend their gratitude to all individuals with disabilities in Ardabil Province, Iran, and the officials of the Ardabil Welfare Organization for their collaboration in this study.
Assistive technologies encompass a range of tools and services designed to support people with chronic conditions, disabilities, elderly individuals, and those facing temporary or permanent impairments [1]. Through a variety of tools and services, these technologies enhance independence and social participation for these groups. Examples of assistive technologies include wheelchairs, hearing aids, white canes, text-to-speech software, and medication organizers [2].
According to a report by the World Health Organization (WHO), 15% of the global population lives with a disability [3]. Additionally, approximately 2.5 billion people rely on assistive technologies to lead a better and more independent life. This number is expected to rise to 3.5 billion by 2050 due to an aging population and the increasing prevalence of non-communicable diseases [4]. Given Iran’s estimated population of around 91.5 million in 2024 [5], an estimated 13.7 million people in the country will experience a disability.
Hence, ensuring access to accessible, appropriate, and affordable assistive technologies is a fundamental human right and a public health and development priority [6]. Moreover, bridging existing gaps is crucial for achieving the sustainable development goals and ensuring the effective implementation of the convention on the rights of persons with disabilities [3].
Despite the widespread need for and positive impact of assistive technologies, access remains significantly limited. Evidence suggests that 90% of individuals in need of assistive technologies are unable to obtain them [3]. However, if the provision of these technologies does not take users’ needs and preferences into account, they may fail to deliver a satisfactory experience. This mismatch can lead to improper use or even abandonment of these technologies [7]. Therefore, aligning assistive technologies with users’ needs and preferences is crucial for their adoption and effectiveness [8].
Various assessment tools have been developed to evaluate user satisfaction and the impact of assistive technologies on functional outcomes, facilitating decision-making and monitoring their use [9]. These tools help improve product design, advance scientific research, shape public policies, and emphasize the importance of assistive technologies in sustaining rehabilitation programs [9, 10].
Despite the critical need for standardized assessment tools, Iran lacks a reliable method for evaluating how well assistive technologies meet the needs of individuals with disabilities. Although the rapid assistive technology assessment tool has been translated into Persian and its face validity has been established, its primary purpose is to assess the prevalence of assistive technology use and needs in the population [11]. This study aims to translate and adapt the consumer form of the ATD-PA and to assess its validity and reliability for adults with disabilities in Iran.
Materials and Methods
This study employed a methodological research design and was conducted in 2023–2024. The target population included adults with disabilities receiving support from the Welfare Organization of Ardabil Province, Iran, and using assistive technology devices. Non-probability quota sampling was employed.
To ensure proper representation, coordination was made with the General Directorate of the Welfare Organization of Ardabil Province, Iran, and the study population was categorized according to the number of assistive technology users in four counties of Ardabil Province (cities of Ardabil, Parsabad, Khalkhal, and Namin). The sample distribution for each county is presented in Table 1.
Inclusion and exclusion criteria
The inclusion criteria were as follows: the individual must have a disability classified as severe or very severe by the Welfare Organization’s medical-rehabilitation commission and be receiving support from the Welfare Organization in Ardabil Province, Iran. Additionally, the individual must be over 18 years old, willing to participate in the research, and able to communicate in Persian. Meanwhile, the individual must also have used at least one assistive technology in the past two months. Subsequently, the exclusion criterion was incomplete questionnaire responses.
Study instruments
In this study, the Assistive Technology Device Predisposition Assessment (ATD PA) was used. Designed by Marcia J. Scher in 1996, this tool assesses the best match between an individual and assistive technology for people over 18 years old [12]. It is part of the matching person and technology (MPT) model, which examines the individual’s characteristics, environment, and technology. The MPT model is based on the International Classification of Functioning, Disability, and Health (ICF) framework, and its goal is to provide a comprehensive evaluation of users’ goals, preferences, environmental factors, and assistive technology [12].
The ATD-PA consists of two forms: one for consumers (users) and one for professionals. The consumer form contains four sections. The first section evaluates individuals’ performance across nine functional domains, including thinking, decision-making and remembering, seeing, hearing, speaking and communicating, muscle power and physical endurance, control of arms, shoulders, trunk, grasping and control of fingers, control of hips, legs, feet, and control of voluntary movement. This section uses a 5-point Likert scale to score responses. The second section evaluates activities, participation, and quality of life through 12 questions, with the average score representing overall quality of life. The third section assesses psychological, social, and emotional characteristics using 32 statements, which are scored accordingly. The fourth section, known as the device form, evaluates consumers’ expectations of the assistive technology they use, based on 12 questions. This tool helps create a consumer profile, enabling rehabilitation professionals to identify functional areas that need intervention [12].
In assessing the internal consistency of the quality-of-life subscale (Section B) of the original ATD-PA version, a Cronbach α of 0.80 indicated good reliability [8]. In studies conducted by the author in 2005 and 2010, the ATD-PA’s high internal consistency and predictive validity were confirmed [13, 14]. Furthermore, a strong correlation between the ATD-PA and the life satisfaction scale was found (Spearman’s Ρ=0.89) [14].
Implementation method
Permission to use the tool was initially obtained from the questionnaire’s designer. The translation process followed the forward-backward method, adhering to the WHO’s recommended standards [15]. First, the tool was translated from English into Persian by a bilingual translator. Next, a back-translation into English was performed by another bilingual translator, who had no previous knowledge of the original. This ensured the accurate conveyance of core concepts and content. The two versions were reviewed in collaboration with rehabilitation and assistive technology experts, incorporating their feedback to finalize the translation. The newly translated English version was then sent to the original author of the questionnaire for review. After receiving approval for conceptual equivalence and consistency with the original, the final Persian version was reviewed by rehabilitation specialists and individuals with disabilities to assess face and content validity.
Two indices, namely content validity ratio (CVR) and content validity index (CVI), were used for quantitative content validity assessment. After collecting the survey questionnaires, expert feedback was analyzed statistically based on CVR and CVI values, resulting in modifications, such as item removal, addition, or revision. The Lawshe method was used to calculate the CVR and determine content validity [16]. Fifteen rehabilitation specialists evaluated the Persian version, rating each item as “essential,” “useful but not essential,” or “not necessary.” Experts also assessed each item’s clarity and relevance. Items with a CVR<0.49 were eliminated. For CVI assessment, specialists evaluated each item for clarity, simplicity, and relevance according to Waltz and Bausell’s guidelines [17]. The percentage of experts selecting the top two categories was then calculated. Items scoring <0.70 were rejected, those between 0.70 and 0.79 required revision, and those >0.79 were deemed acceptable.
Face validity was assessed by collecting feedback from 6 experts and individuals with disabilities on the comprehensibility of the tool’s questions. Revisions were made based on their suggestions.
Factor analysis was conducted to assess the construct validity of the ATD-PA tool. Sample size was determined based on scientific recommendations, suggesting 5 to 10 participants per item [18] and a minimum of 200 participants for factor analysis [19]. Given the 66 items in the tool, a sample of 330 participants was selected for the construct validity assessment. Data adequacy for factor analysis was assessed using the Kaiser-Meyer-Olkin index and the Bartlett test. The varimax rotation method was used to facilitate factor interpretation [20]. The purpose of these analyses was to identify the underlying factors within the items.
The tool’s reliability was assessed through internal consistency and test-retest reliability measures. Due to structural differences among the four sections and the absence of a definitive theoretical model for each, confirmatory factor analysis was not conducted for the ATD-PA tool. Internal consistency was assessed using the Cronbach α coefficient.
Following approval from the Ardabil Welfare Organization and participant selection based on eligibility criteria from the Armaghan system, participant conditions were confirmed via phone calls. Informed consent was then obtained from individuals with disabilities for study participation. Participants attended welfare centers in various counties, where the researcher provided detailed instructions on completing the questionnaire. The participants then completed the ATD-PA tool.
In the final stage, test-retest reliability was assessed by having 30 individuals with disabilities complete the questionnaire again after two weeks. The intraclass correlation coefficient (ICC) was then calculated with a 95% confidence interval (CI).
Statistical analysis
Descriptive statistics were used to summarize participant characteristics, and data analysis, including factor analysis, was performed using SPSS software, version 23.
Results
A total of 330 individuals participated in this study, 57.8% of whom were male. The participants’ Mean±SD age was 43±12.61 years . The largest age group was 31–40 years, representing 25.5% of the participants. Additionally, 45.1% of participants had mobility impairments, and 11.21% used more than two assistive technology devices. The distribution of participant characteristics is presented in Table 2.
In Table 3, the CVR and CVI for the ATD-PA tool were calculated and analyzed. The results indicated that CVR=0.94 and CVI=0.95, both demonstrating a very high level of content validity for this assessment tool.
Exploratory factor analysis for Section B (activity and participation or quality of life) of the questionnaire, consisting of 12 items, was conducted using the maximum likelihood method with varimax rotation. The analysis identified two latent factors: physical health and personal independence, and social interactions and community participation. The Kaiser-Meyer-Olkin measure for this section was 0.884, indicating adequate data for factor analysis. Additionally, the Bartlett test (χ²=973.03, P<0.001) confirmed significant correlations among the items. Based on these findings, the two identified factors accounted for 34.5% of the total variance, with Factor 1 explaining 20.3% and Factor 2 explaining 14.2%. The item loadings for each factor are presented in Table 4.
Exploratory factor analysis for Section D (device form) of the questionnaire, consisting of 12 items, was performed using the maximum likelihood method with varimax rotation. The analysis identified two latent factors: usability and personal compatibility, and social and environmental comfort. The Kaiser-Meyer-Olkin value for this section was 0.865, indicating the adequacy of the data for factor analysis. Additionally, Bartlett’s test (χ²=1066.96, P<0.001) showed significant correlations among the items. Based on the results, the two identified factors explained 37.1% of the total variance in the scores, with the first factor explaining 22.3% and the second factor explaining 14.8%. The items for each factor and their factor loadings are presented in Table 5.
The reliability results of the test, including the intraclass ICCs and the Cronbach α values, are shown in Table 6.
Discussion
To develop the Persian version of the ATD-PA scale, a multi-step process was followed, including initial translation, version unification, and back-translation into the original language. The final version was refined through multiple review sessions by the research team, followed by assessments of face validity, content validity, and construct validity.
In the face validity assessment, no items were eliminated. However, based on expert feedback, modifications were made to items 41 and 63 to 66. Content validity was confirmed with a CVR of 0.94 and a CVI of 0.95, demonstrating the accuracy and precision of the questions in measuring the intended characteristics. These findings align with international studies. In Brazil, the conceptual, semantic, and operational adaptation of the ATD-PA tool was validated with high expert agreement [21]. Similarly, in Germany, strong content validity for this tool was reported, highlighting its reliability in evaluating assistive technologies [22].
Regarding construct validity, the study revealed that while some underlying factors were identified, the explained variance for Sections B (activity and participation or quality of life) and D (device form) was below 50%, indicating the need for revision in these sections. Some of our findings contrast with international studies. For instance, a study in Greece reported satisfactory construct validity for subscales such as adaptability, usability, and satisfaction with assistive technology [23]. Additionally, in this study, Section A (performance) showed a low Cronbach α of 0.235, and Section C (psychosocial characteristics) had a KR-21 value of 0.447, indicating weak reliability. As a result, factor analysis was not conducted for these sections.
In the test, re-test reliability assessment, the ICC values for all sections, measured over a two-week interval, were notably high, ranging from 0.957 to 0.982. These results reflect strong agreement and reliability across all sections, which is consistent with international studies, such as those in Greece (ICC=0.981) and Italy (ICC=0.981) [23, 24].
The obtained Cronbach α values for Section B (0.807) and Section D (0.822) indicate good internal consistency, which aligns with reports from Italy (α=0.702–0.804) [24] and the United States (α=0.80) [13]. These results also correspond with findings from Alves et al. in Brazil, who reported moderate to excellent reliability for the ATD-PA tool [21]. However, the low Cronbach α for Section A (0.235) suggests that the structure of the questions assesses different dimensions within each section. Although the Cronbach α for Section C was not reported, its high ICC (0.982) indicates strong agreement.
The availability of appropriate tools for evaluating the compatibility of assistive technologies with users can have a positive impact on their lives, fostering technological advancements and improving service delivery [25]. These tools not only assess user satisfaction and functional improvements but also measure the impact of assistive technology use over a specified period [9].
The ATD-PA tool has been used in previous research to evaluate the capabilities of assistive technologies across various populations, demonstrating its scientific validity [12].
Conclusion
The Persian version of the ATD-PA demonstrates acceptable psychometric properties for evaluating the experiences of individuals using assistive technologies. Therefore, like the original version, the Persian adaptation is a reliable and valid tool suitable for both clinical and research settings.
Study limitations
Due to the large number of items in this scale and the time required for completion, some rehabilitation service providers, including the Welfare Organization, faced time and resource constraints. These challenges may hinder the creation of comprehensive user profiles, potentially impacting the accuracy and efficiency of assessments. Additionally, reliance on self-reporting by users could reduce evaluation accuracy, as some participants may find it difficult to fully articulate their experiences.
Ethical Considerations
Compliance with ethical guidelines
Informed consent was obtained from participants or their legal guardians. Ethical principles were strictly adhered to, ensuring confidentiality and privacy. Participation was entirely voluntary, and individuals could withdraw from the study at any stage without consequences. This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1402.082).
Funding
This article is derived from Soheila Seyedi’s master’s thesis, which was approved by the Rehabilitation Management Department at the University of Social Welfare and Rehabilitation Sciences. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Methodology, validation, analysis, editing, and finalization, conceptualization, investigation, literature Review, and Manuscript Drafting: All authors; Visualization, supervision, and project management: Kianoush Abdi; Funding Acquisition: Soheila Seyedi.
Conflict of interest
The authors declare no conflicts of interest.
Acknowledgments
The authors extend their gratitude to all individuals with disabilities in Ardabil Province, Iran, and the officials of the Ardabil Welfare Organization for their collaboration in this study.
Refrences
- World Health Organization (WHO). Assistive technology in the Eastern Mediterranean Region: results of a rapid assessment. Genava: World Health Organization; 2019. [Link]
- World Health Organization (WHO). Priority ssistive products list: Improving access to assistive technology for everyone, everywhere. Genava: World Health Organization; 2016. [Link]
- World Health Organization (WHO). Assistive technology [Internet]. 2024 [Updated 2024 January 2]. Available from: [Link]
- World Health Organization (WHO). World report on disability [Internet]. 2011 [Updated 2011 January 1]. Available from: [Link]
- UNdata. World Population Prospects. Iran - Total population (both sexes combined). New York: UNdata; 2024. [Link]
- Toro-Hernández ML, Kankipati P, Goldberg M, Contepomi S, Tsukimoto DR, Bray N. Appropriate Assistive Technology for Developing Countries. Physical medicine and rehabilitation clinics of North America. 2019; 30(4):847-65. [DOI:10.1016/j.pmr.2019.07.008] [PMID]
- Scherer M. “Matching person & technology (MPT) model” for technology selection as well as determination of usability and benefit from use; 2018. [Link]
- Scherer MJ, Cushman LA. Measuring subjective quality of life following spinal cord injury: A validation study of the assistive technology device predisposition assessment. Disability and Rehabilitation. 2001; 23(9):387-93. [DOI:10.1080/09638280010006665] [PMID]
- Alves AC, Matsukura TS, Scherer MJ. Cross-cultural adaptation of the assistive technology device - Predisposition assessment (ATD PA) for use in Brazil (ATD PA Br). Disability and Rehabilitation Assistive Technology. 2017; 12(2):160-4. [DOI:10.1080/17483107.2016.1233294] [PMID]
- Pfaeffli L, Maddison R, Jiang Y, Dalleck L, Löf M. Measuring physical activity in a cardiac rehabilitation population using a smartphone-based questionnaire. Journal of Medical Internet Research. 2013; 15(3):e61. [DOI:10.2196/jmir.2419] [PMID]
- Gerivani H, Takian A, Sajadi HS, Shirazikhah M, Joghataei MT. Translation of the rapid assistive technology assessment tool and assessing its face validity. Archives of Rehabilitation. 2024; 25(3):464-75. [DOI:10.32598/RJ.25.3.2572.4]
- Zap SA. Evidence-based assessment framework for assistive technology: The MPT and MATCH-ACES assessments. Boca Raton: CRC Press; 2023. [Link]
- Scherer MJ, Sax C, Vanbiervliet A, Cushman LA, Scherer JV. Predictors of assistive technology use: the importance of personal and psychosocial factors. Disability and Rehabilitation. 2005; 27(21):1321-31. [DOI:10.1080/09638280500164800] [PMID]
- Scherer MJ, Sax C. Measures of assistive technology predisposition and use. In: Mpofu E, Oakland T, editors. Rehabilitation and health assessment: Applying ICF guidelines. New York: Springer Publishing Co; 2010. [Link]
- Cruchinho P, Franco MD, Capelas M, Almeida S, Bennett P, Silva M, et al. Translation, Cross-Cultural Adaptation, and Validation of Measurement Instruments: A Practical Guideline for Novice Researchers. Journal of Multidisciplinary Healthcare. 2024; 17:2701-28. [DOI:10.2147/JMDH.S419714] [PMID]
- Romero Jeldres M, Díaz Costa E, Faouzi Nadim T. A review of Lawshe’s method for calculating content validity in the social sciences. Frontiers in Education. 2023; 8:1271335. [DOI:10.3389/feduc.2023.1271335]
- Waltz CF, Bausell BR. Nursing research: design statistics and computer analysis. Philadelphia: Davis Fa; 1981. [Link]
- Newman DA. Missing data: Five practical guidelines. Organizational Research Methods. 2014; 17(4):372-411. [DOI:10.1177/1094428114548590]
- Comrey AL, Lee HB. A first course in factor analysis. New York: Psychology Press; 2013. [DOI:10.4324/9781315827506]
- Akhtar-Danesh N. Impact of factor rotation on Q-methodology analysis. Plos One. 2023; 18(9):e0290728. [DOI:10.1371/journal.pone.0290728] [PMID]
- de Jesus Alves AC, Fachin-Martins E. Reliability of assistive technology device-predisposition assessment (ATD PA Br) in Brazilian portuguese. Journal of Occupational Therapy of University of São Paulo. 2018; 29(2):144-54. [Link]
- Bruckmann N, Cordes A, Cam LL, Paland S, Schlegel J, Signoroni J. MPT & ATD PA: Matching person and technology model (MPT-Modell) und assistive technology device predisposition assessment (ATD PA). Idstein: Schulz-Kirchner Verlag GmbH; 2014. [Link]
- Koumpouros Y, Papageorgiou E, Karavasili A. Development of a new psychometric scale (PYTHEIA) to assess the satisfaction of users with any assistive technology. Paper presented in: Advances in Human Factors and Ergonomics in Healthcare: Proceedings of the AHFE 2016 International Conference on Human Factors and Ergonomics in Healthcare. 27July 2016; Orlando: USA. Springer International Publishing, 2017. [DOI:10.1007/978-3-319-41652-6_32]
- Federici S, Scherer M, Ehrlich-Jones L. Measurement characteristics and clinical utility of the assistive technology device predisposition assessment (ATD PA) among mixed patient populations. Archives of Physical Medicine and Rehabilitation. 2021; 102(4):805-806. [DOI:10.1016/j.apmr.2020.11.007]
- Seok S, DaCosta B. Development and standardization of an assistive technology questionnaire using factor analyses: Eight factors consisting of 67 items related to assistive technology practices. Assistive Technology. 2014; 26(1):1-14. [DOI:10.1080/10400435.2013.778917] [PMID]
Type of Study: Applicable |
Subject:
Rehabilitation Management
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
