

Volume 26, Issue 1 (Spring 2025)
jrehab 2025, 26(1): 88-117 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khashaman F, Bahmani B, Harouni G G. Development and Investigating of the Validity and Reliability of Empty Nest Syndrome Questionnaire Among the Elderly. jrehab 2025; 26 (1) :88-117
URL: http://rehabilitationj.uswr.ac.ir/article-1-3367-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3367-en.html



1- Department of Counseling, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. , fkhashaman6@gmail.com
2- Department of Counseling, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Social Welfare, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Counseling, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Social Welfare, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 3063 kb]
(1329 Downloads)
| Abstract (HTML) (5474 Views)
Full-Text: (1553 Views)
Introduction
The aging of the global population represents a significant demographic, medical, and social challenge worldwide [1]. Aging is closely linked with psychological and social processes. Studies have shown that loneliness and social isolation among the elderly have severe negative effects on their mental and physical health. On the other hand, this life stage may be accompanied by various issues, such as hypertension, depression, disabilities due to chronic illnesses, decreased ability to perform previous activities, and reduced income [2]. One of the mental health threats in families that occurs over time, especially as parents enter middle age and old age, is the empty nest syndrome. This syndrome encompasses feelings of loneliness, pervasive sadness, and enduring grief that some parents may experience when their children leave home [3]. It is a psychological condition that can affect one or both parents. When children leave their parental home, parents might experience feelings of sadness, fear, incapacity, role adjustment issues, and changes in parent-child relationships [4]. Research indicates that parents suffering from empty nest syndrome experience a sense of loss that could lead them towards depression and evoke feelings, such as anxiety and loss of life goals [5]. This anxiety can increase parents’ worries about the future, thereby intensifying their loneliness. In other families, marital conflicts overshadowed by child-rearing become evident once the children leave the home. In such cases, the absence of children can lead to increased marital conflicts [6]. As soon as the children leave, couples redefine their lives and relationships, which depending on their responses, might lead to depression [7].
Parents can experience empty nest syndrome either as a physiological or emotional reaction to the departure of their last child from home. The nature of this reaction varies depending on how they approach this natural phase of life, which can be either positive or negative [8]. While empty nest syndrome can be associated with cardiovascular diseases, diabetes, malnutrition, postmenopausal syndrome, decreased sexual intimacy, and aggravation of these conditions, it does not always lead to negative reactions. For some parents, being in an empty nest situation due to increased personal space, more opportunities for self-care, revitalization of marital intimacy, and expansion of social circles can be seen as an opportunity and advantage [9]. Researchers have shown that parents (especially mothers) may suffer harmful consequences such as depression, alcoholism, and identity crisis when their children leave home. However, a rational evaluation suggests that a set of other factors, such as the quality of social relationships, a sense of competence and internal worth, personality type, and physical and psychological health should also be significantly considered [7] Women who have primarily engaged in housework might feel they have lost their role following their children’s marriage. These individuals’ social activities are limited, and they suffer more from empty nest syndrome, depression, and related substance abuse disorders [10]. Moreover, the negative psychological impact of empty nest syndrome is significantly greater in widowed and divorced women because they lack emotional support from a spouse or partner [5]. Thus, empty nest syndrome does not affect all parents equally [4].
Urbanization is currently a major global phenomenon causing an increase in empty nest syndrome, weakening family relationships, and decreasing the quality of life (QoL) for parents living away from their children. As younger generations pursue various opportunities in urban environments, the isolation of parents in rural areas increases, ultimately reducing communication between parents and their children [11]. Additionally, according to the intergenerational solidarity theory in early life, children’s economic needs determine their closeness to their parents. Later in life, parents’ economic needs and health significantly influence the closeness of children to them. However, urbanization in modern society has halted this adjustment, inevitably leading to the weakening of family relationships [12]. The phenomenon of empty nest syndrome is increasingly growing, becoming a significant social issue, and confronting the elderly population with considerable problems, including feelings of loneliness and depression. Furthermore, the prevalence of this syndrome among the middle-aged and elderly population (especially women) is due to the decreasing youth population and increasing elderly population [13]. As the number of single-child families is increasing, it is predicted that the prevalence of this syndrome will exceed 90% by 2030. Moreover, with increasing life expectancy, the prevalence of empty nest syndrome has also increased in Europe and America. A study in the USA showed that 46% of parents experience empty nest syndrome when their children leave home [14].
In 2011, Mbeez and Equando conducted a study examining the effects of empty nest syndrome on parents’ adaptive patterns, which included 91 participants (45 men and 46 women) aged between 45 and 87 years, with an average age of 66 years. The data were collected using an empty nest syndrome questionnaire developed by the researchers, divided into three sections based on a 5-point Likert scale. The questionnaire consisted of three parts. The first part included demographic information of the samples such as the number of children, marital status, gender, and age. The second part, consisting of 16 items, covered feelings related to empty nest syndrome, and finally, the third part focused on parents’ adaptive patterns with 13 items. The Cronbach α coefficient for the questionnaire was 0.81. The authors concluded that empty nest syndrome is significantly related to the adaptive patterns of the elderly, but no significant relationship was found between empty nest syndrome and adaptive patterns due to variables such as gender and family size [15].
In the current research, the most relevant studies in both domestic and international fields since 2010 were reviewed, with the most significant critique being the criteria for including subjects in domestic studies. Specifically, researchers have evaluated parents’ susceptibility to empty nest syndrome based solely on the departure of their child(ren) from home, which has not been objectively investigated. As a result, research findings may be erroneous because not all parents will suffer from empty nest syndrome after their children leave. In international studies, the main and only criterion for study participation considered parents whose children had left home, and in some cases, the symptoms of empty nest syndrome were examined through qualitative interviews with the subjects. Additionally, the only cases where the empty nest syndrome questionnaire was used were in the study conducted by Meez and Equando, which measured the syndrome among middle-aged parents. Despite repeated attempts by the author to access the mentioned questionnaire, it was not possible, and the original file of the empty nest syndrome tool developed by Meez and Equando was not accessible.
From the perspective of justifying the choice of the elderly population instead of middle-aged individuals, which has been the subject of most previous studies, factors such as postmenopausal symptoms in women, retirement, disruption in physical and mental functions, approaching the end of life, and the use of various medications can make this psychological condition a more serious challenge compared to parents in middle age. Additionally, concerns about death are more prominent among the elderly [16], who experience death anxiety more than others [17]. Moreover, in old age, feelings of loneliness are more pronounced compared to other life stages, and determinants of loneliness are more evident among the elderly. This age group, due to experiencing losses such as the death of a spouse, decline in physical function, and health issues, is more involved with the phenomenon of loneliness [18]. Studies have shown that loneliness is significantly associated with higher levels of depression, poor overall health status, functional impairments, increased blood pressure, risk of suicide, and mortality [19]. As one of the most important components of empty nest syndrome is the loneliness of parents, early and objective assessment of this syndrome using an appropriate and effective tool is necessary and practical for supporting and implementing targeted therapeutic interventions in the elderly population.
Materials and Methods
The current research was a psychometric study aimed at constructing, validating, and assessing the reliability of an empty nest syndrome questionnaire among the elderly, conducted cross-sectionally in 2021. The research population included all elderly residents of Tehran City, Iran, who had been left by their children due to migration, employment, education, or marriage in 2021. Field sampling was conducted randomly. For this purpose, the researcher personally visited the homes, assessed the inclusion and exclusion criteria, selected the samples, and completed the questionnaires by the research team. Various factors influence the sample size in tool construction and structural equation modeling studies. For example, more complex models that contain more parameters require a larger sample size [20]. However, generally, a sample size of more than 10 samples per variable is considered appropriate [21]. The sample size in the quantitative part of the study was determined based on the initial conceptual model of the research tool and was finalized after determining the face and content validity, eventually involving 181 participants.
Inclusion and exclusion criteria
The inclusion criteria were as follows: Individuals aged 60 years and above; residents of a household; able to communicate verbally with the researcher; having no psychological disorders interfering with empty nest syndrome; having no severe physical or psychological disabilities that incapacitate them; having no severe physical illnesses and serious sensory or motor impairments that require daily caregiver dependency; not living with children in the same household; no more than three years since the departure of the children from the parent’s home; no experience of a child’s death during these three years. Meanwhile the exclusion criteria were as follows: Spoiled or incomplete questionnaire forms and participant’s withdrawal of consent to participate in the study. To screen for psychological disorders that might interfere with empty nest syndrome, an initial short interview was conducted with the samples. This interview evaluated three main axes: 1) Review of the participant’s history of psychiatric medication use, past and present; 2) Review of the participant’s history of psychological disorders, both past and present; 3) Presence of a life crisis following which the participant had thoughts or plans of suicide. The study was conducted in two phases, each consisting of several steps.
Phase one: Development of items for the empty nest syndrome questionnaire in the elderly
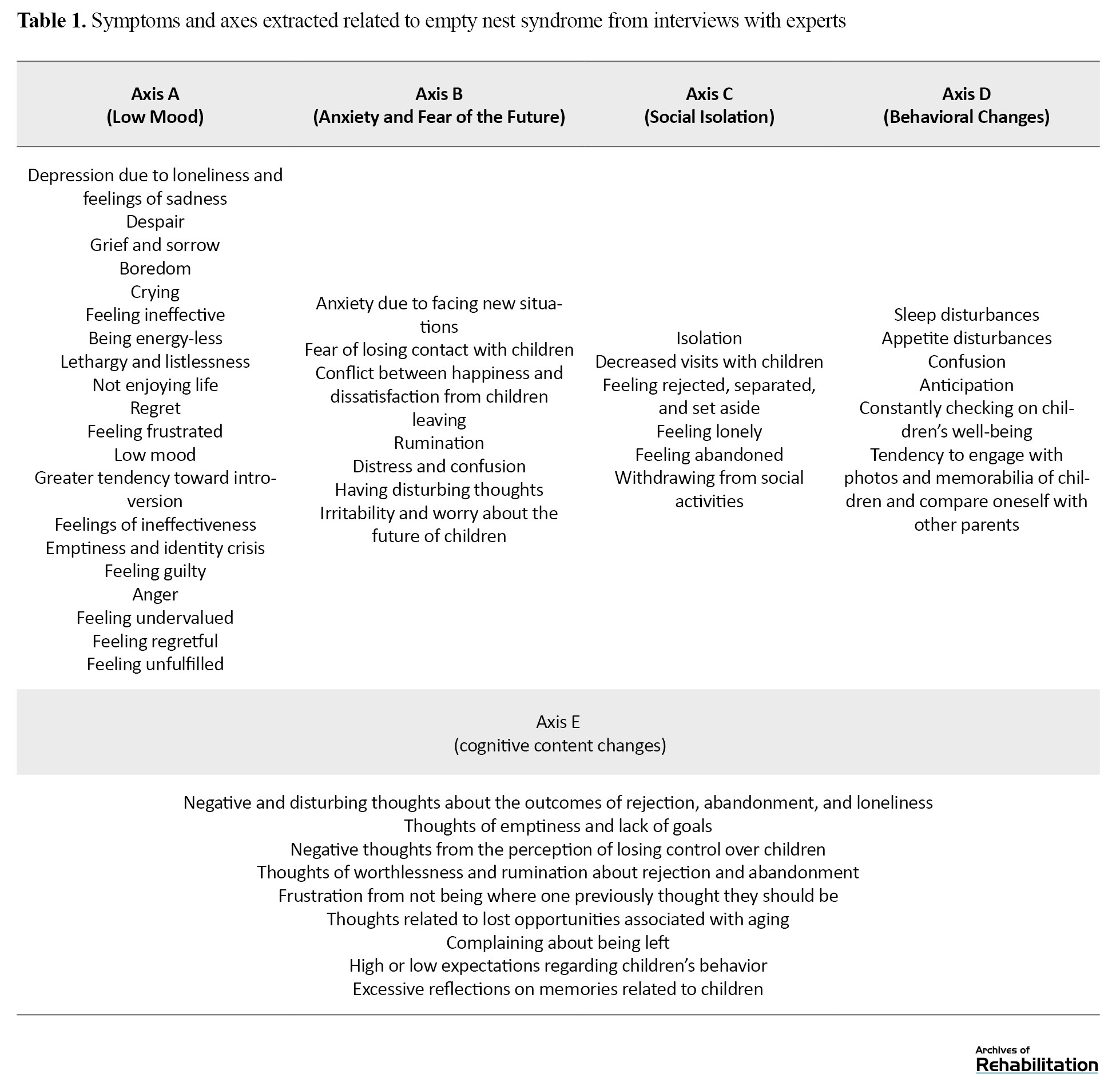
The first step in creating the mentioned tool in this research was to develop a conceptual framework for empty nest syndrome, which was conducted in two stages: 1) Interviews with specialists in psychology, counseling, and gerontology and 2) A review of theoretical resources in domestic and international studies. Interviews were conducted openly and unstructured with six counselors and specialists in psychology and gerontology, and the content was recorded. The duration of interviews ranged from 30 to 85 min, with an average of 45 min. The results of the interviews with the specialists were analyzed using an interpretive analysis method, and the symptoms and signs of empty nest syndrome were matched with the components extracted from the texts in each interview round. The axes extracted in the interviews are mentioned in Table 1.
According to Gilham’s suggestion, to achieve this goal, the interview text should be written in full and detail. The main questions asked, reminders, explorations conducted by the interviewer, and supplementary questions should be mentioned to achieve a complete understanding of what the interviewee has maintained [22].
The second step included using the created theoretical framework and a detailed review of the symptoms of empty nest syndrome, a pool of 40 questions was designed.
The next step involved reviewing, categorizing, eliminating, merging, and modifying the question bank, which was done by the research team in several sessions to create a suitable structure and determine the contribution of each research variable. Ultimately, an initial questionnaire consisting of 40 questions was prepared for presentation to experts for face and content validity assessment.
Phase two: Conducting face and content validity
Assessing face validity
The next step in creating the tool was to assess the validity of the questions, which were measured using various methods. Both qualitative and quantitative methods were utilized to assess face and content validity. Face-to-face interviews with a panel of six experts, presenting the theoretical framework and composition of questions, and obtaining their opinions to find the level of difficulty and deficiencies in the structure of questions and the composition of items, and the importance of item placement in the questionnaire were involved. Subsequently, the revised questions were presented to six experts to assess the appearance, and phrasing, and determine the face validity, where respondents expressed their opinion on each question based on a 5-point Likert scale (very weak, weak, moderate, strong, very strong). During this phase, no questions were eliminated by the expert team based on face validity.
Assessing content validity
To quantitatively calculate content validity, the content validity ratio (CVR) was used to ensure the correctness and importance of the content (necessity of the item). To determine the CVR, the opinion of 6 experts was sought, and they were asked to evaluate the necessity of each item based on a 3-state scale: “Essential,” “useful but not essential,” and “not necessary.” Then, using the Lawshe method (1975) placing the responses in the CVR formula and referring to the table, the necessity of each item was determined [23]. According to Table 1, items that meet the CVR score threshold of 0.99 or higher are eligible for inclusion in the final questionnaire. The used formula is as follows (Equation 1).
In this formula, ne is the number of experts who responded to “essential” and “useful but not essential,” and n is the total number of experts. Based on the number of experts who evaluated the questions, the minimum acceptable CVR value was calculated according to the Lawshe table, and the questions were extracted. The agreed-upon threshold for CVR was set at 0.99 considering the number of experts. Accordingly, in the three sub-scales of the questionnaire, 20 questions met the content validity threshold, and considering the mentioned agreement threshold, another 20 questions that scored below the set threshold were eliminated. After filtering the questions based on face and content validity indices, the finalized questionnaire consisting of 20 items was administered to the target population. After implementing the tool on parents in an empty nest situation, exploratory factor analysis was conducted. In this phase, a team of experts was again formed to discuss the naming of these three sub-scales.
Validity construct of the questionnaire
The construct validity of the research was assessed using the Gerold loneliness scale (convergent validity) and the Keyes positive mental health scale (divergent validity). The Keyes positive mental health scale is derived from the long form of the mental health continuum and includes 14 questions and three components: Emotional well-being, mental health, and social health, assessed on a six-option Likert scale. Scores ranging from 14 to 28 indicate a low level of mental health, scores from 28 to 56 indicate a moderate level of mental health, and scores above 56 indicate a high level of mental health. The reliability of this questionnaire in the current research was determined using the Cronbach α method, which resulted in 0.88 [24].
The Gerold loneliness scale is one of the most widely used tools for measuring loneliness among the elderly and has been utilized in many countries. This tool has few questions, requires less time to complete, and is less likely to cause fatigue in the elderly [25]. The De Jong Gierveld scale has three versions: 34-item, 11-item, and 6-item, with the reliability and validity of the 6-item version conducted in Iran by Hossein Abadi et al. [26]. The Persian version of this tool has acceptable content validity. The results of confirmatory factor analysis indicated a two-factor structure of the questionnaire, consisting of emotional loneliness and social loneliness. The total loneliness score correlated significantly with the hospital anxiety and depression scale. Also, the intraclass correlation coefficient and the Cronbach α coefficient of 0.87 indicated acceptable reliability of the tool.
To identify the number of factors and items related to each factor in the empty nest syndrome questionnaire, exploratory factor analysis (principal component analysis) was used, and factors with eigenvalues above 1 were selected. Given that the best method for achieving a simple orthogonal factor structure is the varimax rotation, this method was deemed suitable for conducting exploratory factor analysis. Moreover, based on the results obtained, it was determined that the sample size reviewed was sufficient for the number of sample groups for factor analysis (Kaiser-Meyer-Olkin=0.895). The test of sphericity by Bartlett was also significant, indicating that this condition was met for factor analysis (P<0.000 and χ²=2597).
Results
This study aimed to create a measurement tool for empty nest syndrome among the Iranian elderly population. The study sample consisted of 181 residents of Tehran City, Iran, over 60 years old, with more than half of the population (68%) being women. In terms of age, all participants are considered young elderly, ranging from 60 to 75 years old. Regarding marital status, 72.4% of the sample live with their spouse, 20.4% are widowed, and less than 10% are divorced. In terms of education, the highest frequency is related to high school and middle school education, each accounting for 20.4%. Regarding economic status, the majority of individuals are at a medium level (51.9%). In terms of employment status, 27.6% of participants are housewives, and only 6% are employed in the private sector and are currently retired. The frequency of face-to-face contact between parents and their children in most samples is once a week (29.8%), while the frequency of non-face-to-face contact is daily, accounting for 51.9%. Based on descriptive findings related to the variable number of children, the highest percentage (27.1) is related to having four children. Regarding housing status, 71.3% of participants own their property. Regarding the time elapsed since the last child left home, most samples, namely 48.1%, are in the first year after their last child left home. Table 2 lists the descriptive statistics of the demographic variables of the participants.
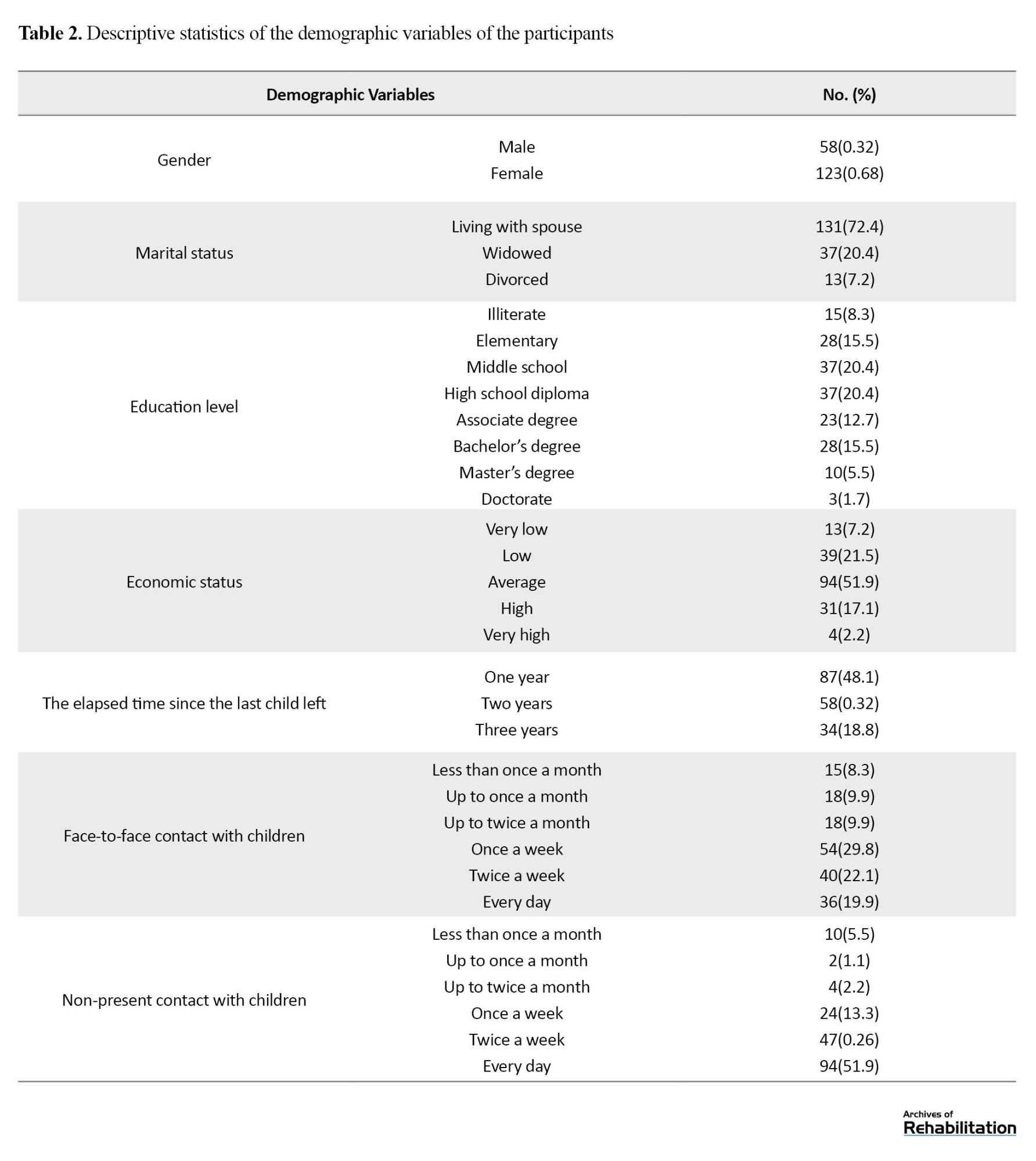
Meanwhile, the demographic information of the samples was self-reported and completed in the form of a questionnaire.
To construct the empty nest syndrome questionnaire, initial scientific studies in the field were reviewed, and in the second step of this phase, interviews were conducted with six specialists, and the symptoms of empty nest syndrome were summarized in five axes. In the next step, we proceeded to design 40 questions based on the themes extracted from interviews with experts. Based on the results obtained from the qualitative and quantitative validity assessment of the tool and the results obtained from the content validity assessment, the questionnaire results were modified as follows:
- Question 7 was removed due to overlap with question 2;
- Question 14 was removed due to overlap with question 19;
- Question 27 measures two different categories and is conceptually flawed, so the decision was made to remove it;
- Questions 40, 39, 36, 35, 31, 32, 33, 29, 28, 24, 25, 22, 13, 5, 8, 9, and 10 were removed due to not meeting the content validity threshold.
After administering the questionnaire to the target population, exploratory factor analysis was performed on the questions, resulting in the extraction of 20 questions under three factors. Due to the lack of conceptual alignment of the items with other questions within the related factor, some questions were removed, ultimately leaving 15 questions. In the first sub-scale, titled “Feeling of Rejection,” question 14 is included. In the second sub-scale, named “fear of losing children,” questions 5 and 7 are included, and finally, in the third sub-scale, termed “social support,” questions 1 and 2 were removed. The Cronbach α coefficient was increased. According to the CVR table in the article text and consistent with the Lawshe threshold, the questionnaire has acceptable content validity. In terms of face validity, the tool has acceptable validity according to the experts. These three factors together explained 72.895% of the total variance. The first factor, with 8 items, includes having a sense of identity loss, feelings of worthlessness, feeling isolated, less inclination to eat, more tendency to cry, being forgotten and set aside by children, and ultimately, the children’s lack of patience to spend time with parents. These factors, with an eigenvalue of 15.728, indicate a very high factor loading of the questions and explain 36.188% of the total variance of the questions. The second factor, with four questions, covers areas such as the fear of losing children, concerns about the future and being left alone, excessive thinking about the children’s situation, and reminiscing about related memories. This dimension, due to its implications for factors causing anxiety in parents, was named “fear of losing children.” The structure of the third factor’s questions, which are of a positive nature, consists of three questions and includes having a good standing, receiving feelings of warmth and support from others, and having people in life to ask for help, thus this dimension was named “Social Support.” Accordingly, based on statistical results, three factors with eigenvalues above 1 were identified as the most significant factors. Ultimately, according to the results of the exploratory factor analysis, it was determined that the 15-item empty nest syndrome questionnaire assesses three factors. Therefore, researchers named the measurement tool for empty nest syndrome in three domains: “Feeling of rejection,” “fear of losing children,” and “social support.”
The coefficients ranged from a minimum of 0.80 to a maximum of 0.93, with an overall α of 0.88, indicating acceptable internal consistency of the tool. Construct validity refers to the degree of correlation and convergence of test scores with scores from other similar validated tests. The concurrent validity of the test is determined through the correlation of test results with outcomes of similar tests conducted simultaneously [27]. For the construct validity of the questionnaire, two aligned and misaligned tools were selected for the empty nest syndrome questionnaire; these include the Gerold loneliness scale (6-item version) and Keyes’s positive mental health questionnaire. According to the research findings, there is a significant negative correlation between the subscales of feeling rejected, social support, and the overall score of the empty nest syndrome questionnaire with the positive mental health tool; in other words, the higher the score obtained in the empty nest syndrome questionnaire, the lower the score in the positive mental health questionnaire. Additionally, there is a significant positive correlation between the social support subscale and the overall score of the empty nest syndrome questionnaire with the overall score of the loneliness scale.
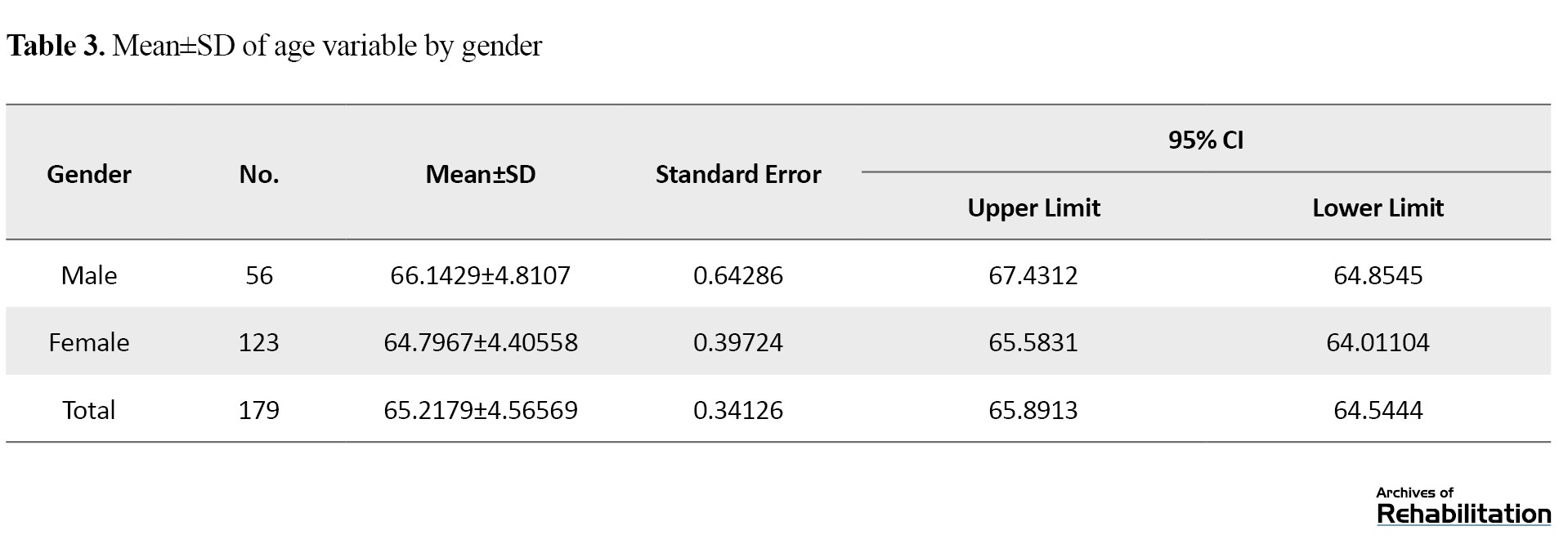
According to the data from the above table, the average age in the male group is 66 years, and in the female group, it is 64 years, with the overall average age being 65 (Table 3).
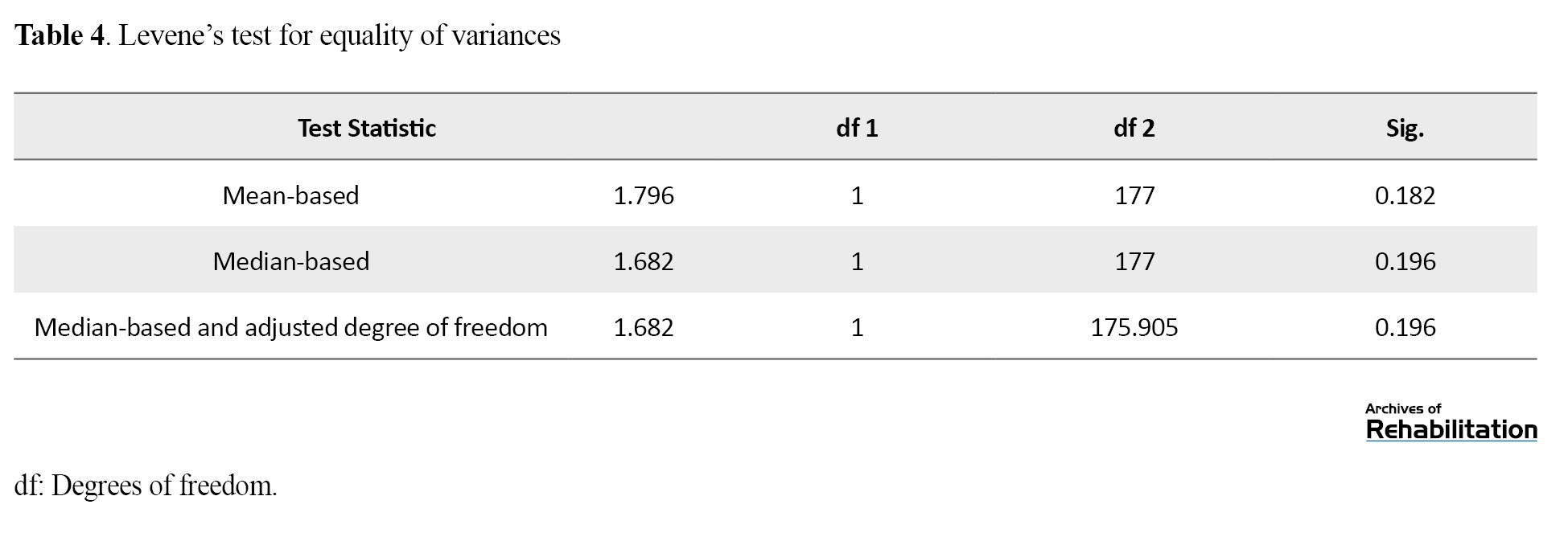
According to the results of the Levene test and as indicated in the above table, since the significance level is 0.182 and greater than 0.05, the variances across groups are considered equal (Table 4).
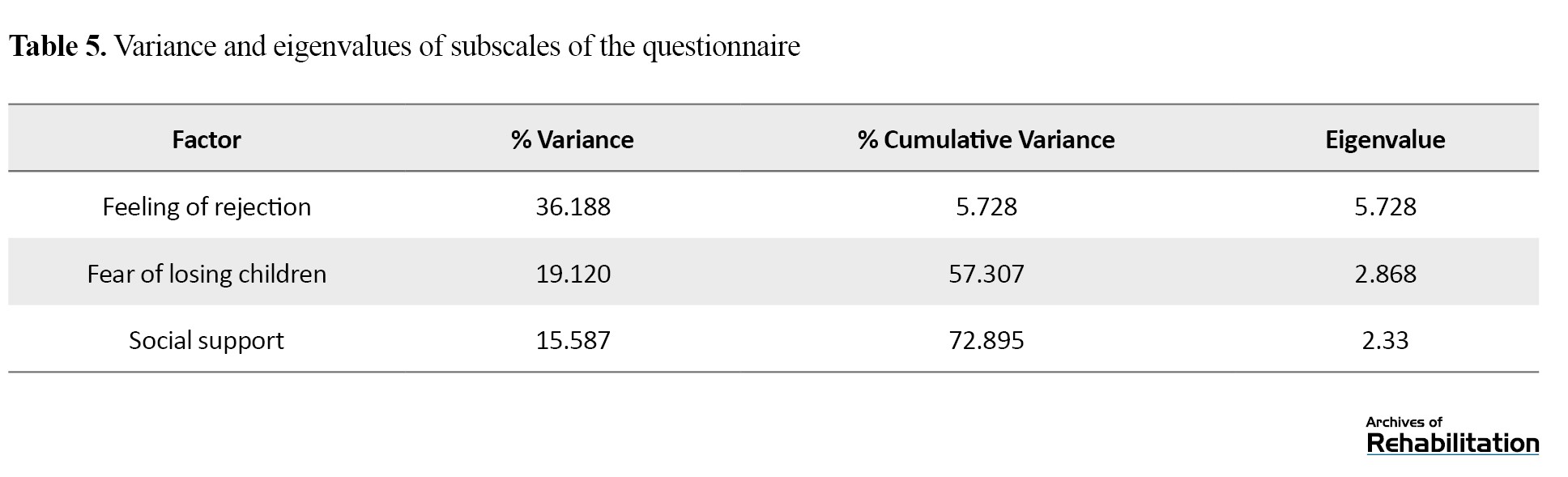
The results of the exploratory factor analysis revealed that three main factors were extracted from the data. These factors include feeling of rejection, fear of losing children, and social support. Each of these factors explained a significant portion of the total variance, and their eigenvalues exceeded the acceptable threshold for factor analysis. These findings confirm the appropriate factorial structure and construct validity of the questionnaire, indicating that the identified dimensions effectively capture the intended concept (Table 5).
To assess the reliability of the questionnaire, Cronbach’s α coefficients were calculated for each dimension as well as for the overall scale. The results indicated that all dimensions demonstrated acceptable to excellent internal consistency. Specifically, the Feeling of Rejection dimension achieved a high reliability coefficient, while the Fear of Losing Children and Social Support dimensions also showed good reliability values. Additionally, the overall Cronbach’s α for the empty nest syndrome questionnaire confirmed the satisfactory internal consistency of the entire tool, indicating that the items within each factor, as well as the whole scale, reliably measure the intended constructs (Table 6).

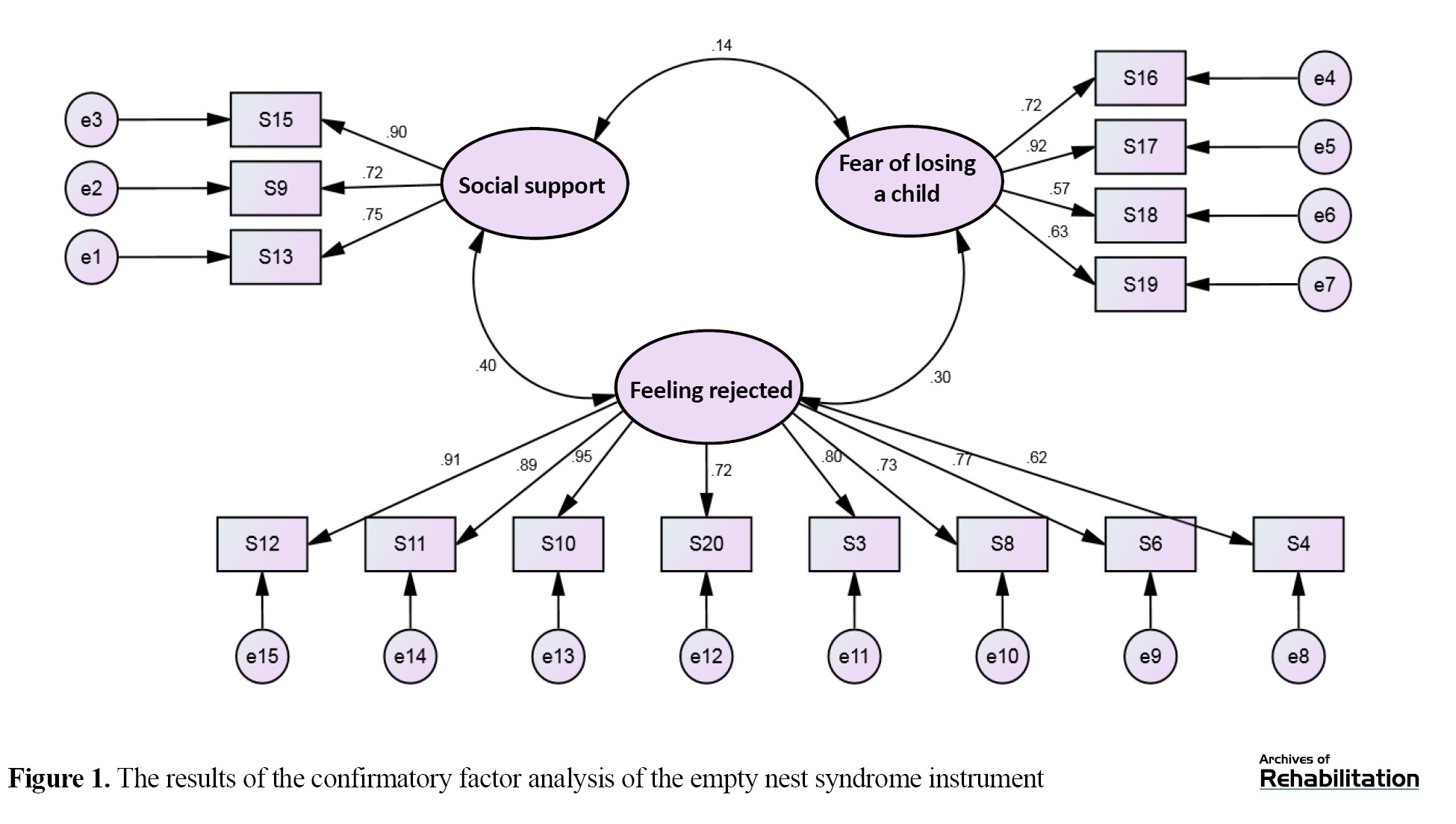
After conducting exploratory factor analysis, confirmatory factor analysis was used to test the fit of the obtained factors using Amos software (Figure 1).
The aging of the global population represents a significant demographic, medical, and social challenge worldwide [1]. Aging is closely linked with psychological and social processes. Studies have shown that loneliness and social isolation among the elderly have severe negative effects on their mental and physical health. On the other hand, this life stage may be accompanied by various issues, such as hypertension, depression, disabilities due to chronic illnesses, decreased ability to perform previous activities, and reduced income [2]. One of the mental health threats in families that occurs over time, especially as parents enter middle age and old age, is the empty nest syndrome. This syndrome encompasses feelings of loneliness, pervasive sadness, and enduring grief that some parents may experience when their children leave home [3]. It is a psychological condition that can affect one or both parents. When children leave their parental home, parents might experience feelings of sadness, fear, incapacity, role adjustment issues, and changes in parent-child relationships [4]. Research indicates that parents suffering from empty nest syndrome experience a sense of loss that could lead them towards depression and evoke feelings, such as anxiety and loss of life goals [5]. This anxiety can increase parents’ worries about the future, thereby intensifying their loneliness. In other families, marital conflicts overshadowed by child-rearing become evident once the children leave the home. In such cases, the absence of children can lead to increased marital conflicts [6]. As soon as the children leave, couples redefine their lives and relationships, which depending on their responses, might lead to depression [7].
Parents can experience empty nest syndrome either as a physiological or emotional reaction to the departure of their last child from home. The nature of this reaction varies depending on how they approach this natural phase of life, which can be either positive or negative [8]. While empty nest syndrome can be associated with cardiovascular diseases, diabetes, malnutrition, postmenopausal syndrome, decreased sexual intimacy, and aggravation of these conditions, it does not always lead to negative reactions. For some parents, being in an empty nest situation due to increased personal space, more opportunities for self-care, revitalization of marital intimacy, and expansion of social circles can be seen as an opportunity and advantage [9]. Researchers have shown that parents (especially mothers) may suffer harmful consequences such as depression, alcoholism, and identity crisis when their children leave home. However, a rational evaluation suggests that a set of other factors, such as the quality of social relationships, a sense of competence and internal worth, personality type, and physical and psychological health should also be significantly considered [7] Women who have primarily engaged in housework might feel they have lost their role following their children’s marriage. These individuals’ social activities are limited, and they suffer more from empty nest syndrome, depression, and related substance abuse disorders [10]. Moreover, the negative psychological impact of empty nest syndrome is significantly greater in widowed and divorced women because they lack emotional support from a spouse or partner [5]. Thus, empty nest syndrome does not affect all parents equally [4].
Urbanization is currently a major global phenomenon causing an increase in empty nest syndrome, weakening family relationships, and decreasing the quality of life (QoL) for parents living away from their children. As younger generations pursue various opportunities in urban environments, the isolation of parents in rural areas increases, ultimately reducing communication between parents and their children [11]. Additionally, according to the intergenerational solidarity theory in early life, children’s economic needs determine their closeness to their parents. Later in life, parents’ economic needs and health significantly influence the closeness of children to them. However, urbanization in modern society has halted this adjustment, inevitably leading to the weakening of family relationships [12]. The phenomenon of empty nest syndrome is increasingly growing, becoming a significant social issue, and confronting the elderly population with considerable problems, including feelings of loneliness and depression. Furthermore, the prevalence of this syndrome among the middle-aged and elderly population (especially women) is due to the decreasing youth population and increasing elderly population [13]. As the number of single-child families is increasing, it is predicted that the prevalence of this syndrome will exceed 90% by 2030. Moreover, with increasing life expectancy, the prevalence of empty nest syndrome has also increased in Europe and America. A study in the USA showed that 46% of parents experience empty nest syndrome when their children leave home [14].
In 2011, Mbeez and Equando conducted a study examining the effects of empty nest syndrome on parents’ adaptive patterns, which included 91 participants (45 men and 46 women) aged between 45 and 87 years, with an average age of 66 years. The data were collected using an empty nest syndrome questionnaire developed by the researchers, divided into three sections based on a 5-point Likert scale. The questionnaire consisted of three parts. The first part included demographic information of the samples such as the number of children, marital status, gender, and age. The second part, consisting of 16 items, covered feelings related to empty nest syndrome, and finally, the third part focused on parents’ adaptive patterns with 13 items. The Cronbach α coefficient for the questionnaire was 0.81. The authors concluded that empty nest syndrome is significantly related to the adaptive patterns of the elderly, but no significant relationship was found between empty nest syndrome and adaptive patterns due to variables such as gender and family size [15].
In the current research, the most relevant studies in both domestic and international fields since 2010 were reviewed, with the most significant critique being the criteria for including subjects in domestic studies. Specifically, researchers have evaluated parents’ susceptibility to empty nest syndrome based solely on the departure of their child(ren) from home, which has not been objectively investigated. As a result, research findings may be erroneous because not all parents will suffer from empty nest syndrome after their children leave. In international studies, the main and only criterion for study participation considered parents whose children had left home, and in some cases, the symptoms of empty nest syndrome were examined through qualitative interviews with the subjects. Additionally, the only cases where the empty nest syndrome questionnaire was used were in the study conducted by Meez and Equando, which measured the syndrome among middle-aged parents. Despite repeated attempts by the author to access the mentioned questionnaire, it was not possible, and the original file of the empty nest syndrome tool developed by Meez and Equando was not accessible.
From the perspective of justifying the choice of the elderly population instead of middle-aged individuals, which has been the subject of most previous studies, factors such as postmenopausal symptoms in women, retirement, disruption in physical and mental functions, approaching the end of life, and the use of various medications can make this psychological condition a more serious challenge compared to parents in middle age. Additionally, concerns about death are more prominent among the elderly [16], who experience death anxiety more than others [17]. Moreover, in old age, feelings of loneliness are more pronounced compared to other life stages, and determinants of loneliness are more evident among the elderly. This age group, due to experiencing losses such as the death of a spouse, decline in physical function, and health issues, is more involved with the phenomenon of loneliness [18]. Studies have shown that loneliness is significantly associated with higher levels of depression, poor overall health status, functional impairments, increased blood pressure, risk of suicide, and mortality [19]. As one of the most important components of empty nest syndrome is the loneliness of parents, early and objective assessment of this syndrome using an appropriate and effective tool is necessary and practical for supporting and implementing targeted therapeutic interventions in the elderly population.
Materials and Methods
The current research was a psychometric study aimed at constructing, validating, and assessing the reliability of an empty nest syndrome questionnaire among the elderly, conducted cross-sectionally in 2021. The research population included all elderly residents of Tehran City, Iran, who had been left by their children due to migration, employment, education, or marriage in 2021. Field sampling was conducted randomly. For this purpose, the researcher personally visited the homes, assessed the inclusion and exclusion criteria, selected the samples, and completed the questionnaires by the research team. Various factors influence the sample size in tool construction and structural equation modeling studies. For example, more complex models that contain more parameters require a larger sample size [20]. However, generally, a sample size of more than 10 samples per variable is considered appropriate [21]. The sample size in the quantitative part of the study was determined based on the initial conceptual model of the research tool and was finalized after determining the face and content validity, eventually involving 181 participants.
Inclusion and exclusion criteria
The inclusion criteria were as follows: Individuals aged 60 years and above; residents of a household; able to communicate verbally with the researcher; having no psychological disorders interfering with empty nest syndrome; having no severe physical or psychological disabilities that incapacitate them; having no severe physical illnesses and serious sensory or motor impairments that require daily caregiver dependency; not living with children in the same household; no more than three years since the departure of the children from the parent’s home; no experience of a child’s death during these three years. Meanwhile the exclusion criteria were as follows: Spoiled or incomplete questionnaire forms and participant’s withdrawal of consent to participate in the study. To screen for psychological disorders that might interfere with empty nest syndrome, an initial short interview was conducted with the samples. This interview evaluated three main axes: 1) Review of the participant’s history of psychiatric medication use, past and present; 2) Review of the participant’s history of psychological disorders, both past and present; 3) Presence of a life crisis following which the participant had thoughts or plans of suicide. The study was conducted in two phases, each consisting of several steps.
Phase one: Development of items for the empty nest syndrome questionnaire in the elderly
The first step in creating the mentioned tool in this research was to develop a conceptual framework for empty nest syndrome, which was conducted in two stages: 1) Interviews with specialists in psychology, counseling, and gerontology and 2) A review of theoretical resources in domestic and international studies. Interviews were conducted openly and unstructured with six counselors and specialists in psychology and gerontology, and the content was recorded. The duration of interviews ranged from 30 to 85 min, with an average of 45 min. The results of the interviews with the specialists were analyzed using an interpretive analysis method, and the symptoms and signs of empty nest syndrome were matched with the components extracted from the texts in each interview round. The axes extracted in the interviews are mentioned in Table 1.
According to Gilham’s suggestion, to achieve this goal, the interview text should be written in full and detail. The main questions asked, reminders, explorations conducted by the interviewer, and supplementary questions should be mentioned to achieve a complete understanding of what the interviewee has maintained [22].
The second step included using the created theoretical framework and a detailed review of the symptoms of empty nest syndrome, a pool of 40 questions was designed.
The next step involved reviewing, categorizing, eliminating, merging, and modifying the question bank, which was done by the research team in several sessions to create a suitable structure and determine the contribution of each research variable. Ultimately, an initial questionnaire consisting of 40 questions was prepared for presentation to experts for face and content validity assessment.
Phase two: Conducting face and content validity
Assessing face validity
The next step in creating the tool was to assess the validity of the questions, which were measured using various methods. Both qualitative and quantitative methods were utilized to assess face and content validity. Face-to-face interviews with a panel of six experts, presenting the theoretical framework and composition of questions, and obtaining their opinions to find the level of difficulty and deficiencies in the structure of questions and the composition of items, and the importance of item placement in the questionnaire were involved. Subsequently, the revised questions were presented to six experts to assess the appearance, and phrasing, and determine the face validity, where respondents expressed their opinion on each question based on a 5-point Likert scale (very weak, weak, moderate, strong, very strong). During this phase, no questions were eliminated by the expert team based on face validity.
Assessing content validity
To quantitatively calculate content validity, the content validity ratio (CVR) was used to ensure the correctness and importance of the content (necessity of the item). To determine the CVR, the opinion of 6 experts was sought, and they were asked to evaluate the necessity of each item based on a 3-state scale: “Essential,” “useful but not essential,” and “not necessary.” Then, using the Lawshe method (1975) placing the responses in the CVR formula and referring to the table, the necessity of each item was determined [23]. According to Table 1, items that meet the CVR score threshold of 0.99 or higher are eligible for inclusion in the final questionnaire. The used formula is as follows (Equation 1).
In this formula, ne is the number of experts who responded to “essential” and “useful but not essential,” and n is the total number of experts. Based on the number of experts who evaluated the questions, the minimum acceptable CVR value was calculated according to the Lawshe table, and the questions were extracted. The agreed-upon threshold for CVR was set at 0.99 considering the number of experts. Accordingly, in the three sub-scales of the questionnaire, 20 questions met the content validity threshold, and considering the mentioned agreement threshold, another 20 questions that scored below the set threshold were eliminated. After filtering the questions based on face and content validity indices, the finalized questionnaire consisting of 20 items was administered to the target population. After implementing the tool on parents in an empty nest situation, exploratory factor analysis was conducted. In this phase, a team of experts was again formed to discuss the naming of these three sub-scales.
Validity construct of the questionnaire
The construct validity of the research was assessed using the Gerold loneliness scale (convergent validity) and the Keyes positive mental health scale (divergent validity). The Keyes positive mental health scale is derived from the long form of the mental health continuum and includes 14 questions and three components: Emotional well-being, mental health, and social health, assessed on a six-option Likert scale. Scores ranging from 14 to 28 indicate a low level of mental health, scores from 28 to 56 indicate a moderate level of mental health, and scores above 56 indicate a high level of mental health. The reliability of this questionnaire in the current research was determined using the Cronbach α method, which resulted in 0.88 [24].
The Gerold loneliness scale is one of the most widely used tools for measuring loneliness among the elderly and has been utilized in many countries. This tool has few questions, requires less time to complete, and is less likely to cause fatigue in the elderly [25]. The De Jong Gierveld scale has three versions: 34-item, 11-item, and 6-item, with the reliability and validity of the 6-item version conducted in Iran by Hossein Abadi et al. [26]. The Persian version of this tool has acceptable content validity. The results of confirmatory factor analysis indicated a two-factor structure of the questionnaire, consisting of emotional loneliness and social loneliness. The total loneliness score correlated significantly with the hospital anxiety and depression scale. Also, the intraclass correlation coefficient and the Cronbach α coefficient of 0.87 indicated acceptable reliability of the tool.
To identify the number of factors and items related to each factor in the empty nest syndrome questionnaire, exploratory factor analysis (principal component analysis) was used, and factors with eigenvalues above 1 were selected. Given that the best method for achieving a simple orthogonal factor structure is the varimax rotation, this method was deemed suitable for conducting exploratory factor analysis. Moreover, based on the results obtained, it was determined that the sample size reviewed was sufficient for the number of sample groups for factor analysis (Kaiser-Meyer-Olkin=0.895). The test of sphericity by Bartlett was also significant, indicating that this condition was met for factor analysis (P<0.000 and χ²=2597).
Results
This study aimed to create a measurement tool for empty nest syndrome among the Iranian elderly population. The study sample consisted of 181 residents of Tehran City, Iran, over 60 years old, with more than half of the population (68%) being women. In terms of age, all participants are considered young elderly, ranging from 60 to 75 years old. Regarding marital status, 72.4% of the sample live with their spouse, 20.4% are widowed, and less than 10% are divorced. In terms of education, the highest frequency is related to high school and middle school education, each accounting for 20.4%. Regarding economic status, the majority of individuals are at a medium level (51.9%). In terms of employment status, 27.6% of participants are housewives, and only 6% are employed in the private sector and are currently retired. The frequency of face-to-face contact between parents and their children in most samples is once a week (29.8%), while the frequency of non-face-to-face contact is daily, accounting for 51.9%. Based on descriptive findings related to the variable number of children, the highest percentage (27.1) is related to having four children. Regarding housing status, 71.3% of participants own their property. Regarding the time elapsed since the last child left home, most samples, namely 48.1%, are in the first year after their last child left home. Table 2 lists the descriptive statistics of the demographic variables of the participants.
Meanwhile, the demographic information of the samples was self-reported and completed in the form of a questionnaire.
To construct the empty nest syndrome questionnaire, initial scientific studies in the field were reviewed, and in the second step of this phase, interviews were conducted with six specialists, and the symptoms of empty nest syndrome were summarized in five axes. In the next step, we proceeded to design 40 questions based on the themes extracted from interviews with experts. Based on the results obtained from the qualitative and quantitative validity assessment of the tool and the results obtained from the content validity assessment, the questionnaire results were modified as follows:
- Question 7 was removed due to overlap with question 2;
- Question 14 was removed due to overlap with question 19;
- Question 27 measures two different categories and is conceptually flawed, so the decision was made to remove it;
- Questions 40, 39, 36, 35, 31, 32, 33, 29, 28, 24, 25, 22, 13, 5, 8, 9, and 10 were removed due to not meeting the content validity threshold.
After administering the questionnaire to the target population, exploratory factor analysis was performed on the questions, resulting in the extraction of 20 questions under three factors. Due to the lack of conceptual alignment of the items with other questions within the related factor, some questions were removed, ultimately leaving 15 questions. In the first sub-scale, titled “Feeling of Rejection,” question 14 is included. In the second sub-scale, named “fear of losing children,” questions 5 and 7 are included, and finally, in the third sub-scale, termed “social support,” questions 1 and 2 were removed. The Cronbach α coefficient was increased. According to the CVR table in the article text and consistent with the Lawshe threshold, the questionnaire has acceptable content validity. In terms of face validity, the tool has acceptable validity according to the experts. These three factors together explained 72.895% of the total variance. The first factor, with 8 items, includes having a sense of identity loss, feelings of worthlessness, feeling isolated, less inclination to eat, more tendency to cry, being forgotten and set aside by children, and ultimately, the children’s lack of patience to spend time with parents. These factors, with an eigenvalue of 15.728, indicate a very high factor loading of the questions and explain 36.188% of the total variance of the questions. The second factor, with four questions, covers areas such as the fear of losing children, concerns about the future and being left alone, excessive thinking about the children’s situation, and reminiscing about related memories. This dimension, due to its implications for factors causing anxiety in parents, was named “fear of losing children.” The structure of the third factor’s questions, which are of a positive nature, consists of three questions and includes having a good standing, receiving feelings of warmth and support from others, and having people in life to ask for help, thus this dimension was named “Social Support.” Accordingly, based on statistical results, three factors with eigenvalues above 1 were identified as the most significant factors. Ultimately, according to the results of the exploratory factor analysis, it was determined that the 15-item empty nest syndrome questionnaire assesses three factors. Therefore, researchers named the measurement tool for empty nest syndrome in three domains: “Feeling of rejection,” “fear of losing children,” and “social support.”
The coefficients ranged from a minimum of 0.80 to a maximum of 0.93, with an overall α of 0.88, indicating acceptable internal consistency of the tool. Construct validity refers to the degree of correlation and convergence of test scores with scores from other similar validated tests. The concurrent validity of the test is determined through the correlation of test results with outcomes of similar tests conducted simultaneously [27]. For the construct validity of the questionnaire, two aligned and misaligned tools were selected for the empty nest syndrome questionnaire; these include the Gerold loneliness scale (6-item version) and Keyes’s positive mental health questionnaire. According to the research findings, there is a significant negative correlation between the subscales of feeling rejected, social support, and the overall score of the empty nest syndrome questionnaire with the positive mental health tool; in other words, the higher the score obtained in the empty nest syndrome questionnaire, the lower the score in the positive mental health questionnaire. Additionally, there is a significant positive correlation between the social support subscale and the overall score of the empty nest syndrome questionnaire with the overall score of the loneliness scale.
According to the data from the above table, the average age in the male group is 66 years, and in the female group, it is 64 years, with the overall average age being 65 (Table 3).
According to the results of the Levene test and as indicated in the above table, since the significance level is 0.182 and greater than 0.05, the variances across groups are considered equal (Table 4).
The results of the exploratory factor analysis revealed that three main factors were extracted from the data. These factors include feeling of rejection, fear of losing children, and social support. Each of these factors explained a significant portion of the total variance, and their eigenvalues exceeded the acceptable threshold for factor analysis. These findings confirm the appropriate factorial structure and construct validity of the questionnaire, indicating that the identified dimensions effectively capture the intended concept (Table 5).
To assess the reliability of the questionnaire, Cronbach’s α coefficients were calculated for each dimension as well as for the overall scale. The results indicated that all dimensions demonstrated acceptable to excellent internal consistency. Specifically, the Feeling of Rejection dimension achieved a high reliability coefficient, while the Fear of Losing Children and Social Support dimensions also showed good reliability values. Additionally, the overall Cronbach’s α for the empty nest syndrome questionnaire confirmed the satisfactory internal consistency of the entire tool, indicating that the items within each factor, as well as the whole scale, reliably measure the intended constructs (Table 6).
After conducting exploratory factor analysis, confirmatory factor analysis was used to test the fit of the obtained factors using Amos software (Figure 1).
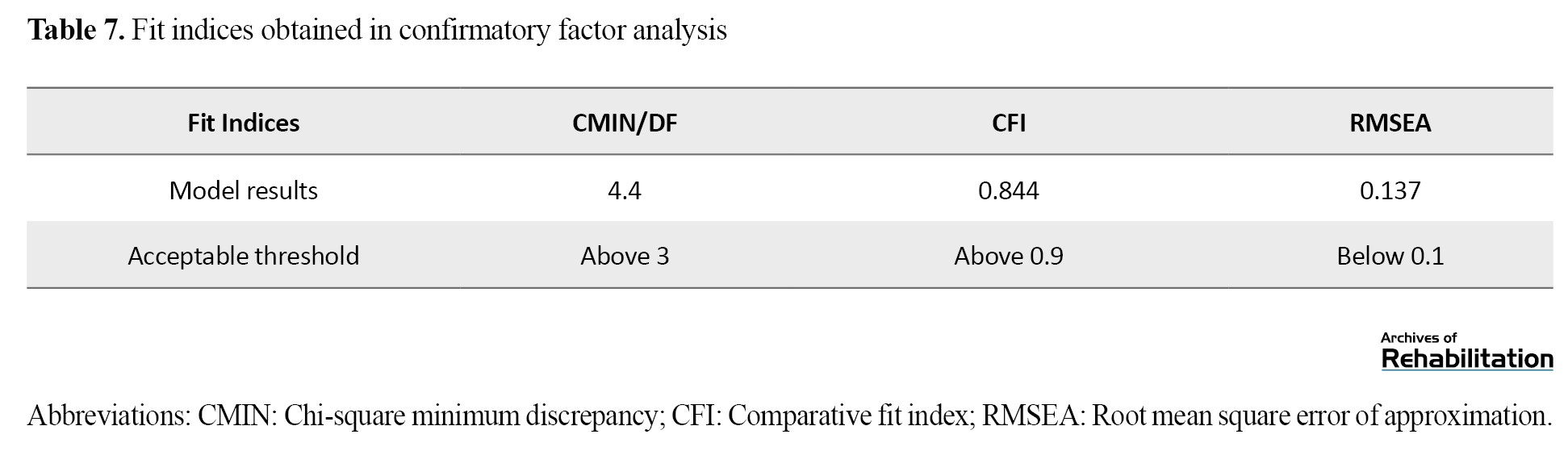
In the confirmatory factor analysis, according to the factor loadings and the obtained fit indices (fit indices resulting from the implementation of the model), it was found that the 15-question empty nest syndrome questionnaire has an acceptable fit. Good fit indices that have reached the required quota are listed in Table 7.
Test re-test reliability (temporal stability)
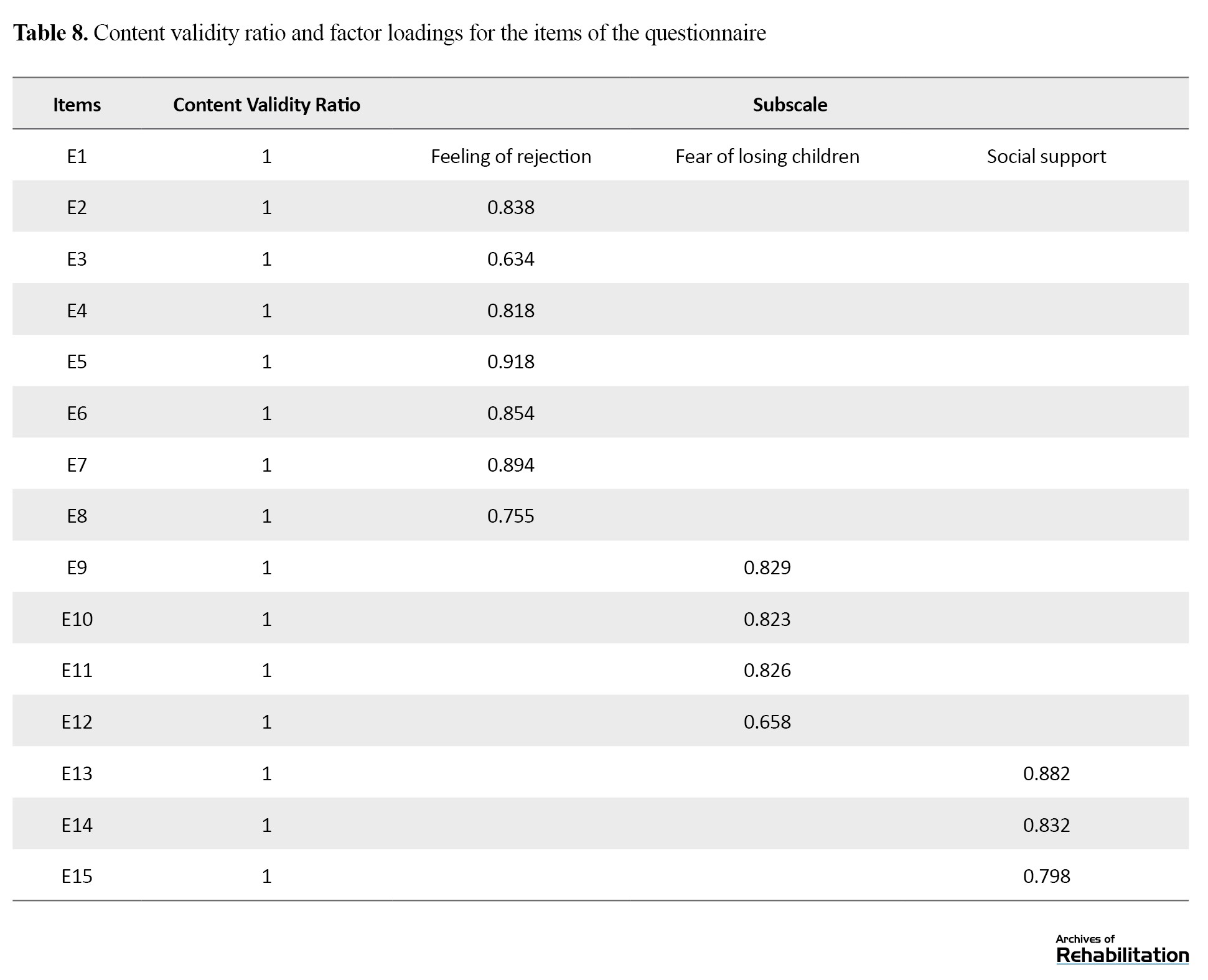
To examine the test ret-est reliability (temporal stability), scores from the questionnaire were correlated across two sessions conducted one week apart with 30 subjects. The results of the study indicated a stability index of 0.994, demonstrating the high reliability of the test. Exploratory factor analysis and reliability assessment of the tool were performed using SPSS software, version 26, and confirmatory factor analysis was conducted using Amos software version 24. This questionnaire consists of 15 questions with a 5-point Likert scale ranging from very low to very high. The tool contains three subscales measuring aspects such as feelings of rejection, fear of losing children, and social support for the elderly. Theoretically, this measure evaluates mild to severe symptoms and feelings of empty nest syndrome. Specifically, the total score of the questionnaire is the sum of the scores in each of the three subscales, resulting in a final score ranging from 1 to 95. Scores ranging from 1 to 33 indicate mild empty nest syndrome, scores from 33.1 to 55 suggest moderate syndrome, and scores from 55.1 to 75 indicate high levels of empty nest syndrome.To evaluate the content validity of the questionnaire, the content validity ratio (CVR) was calculated for each item based on the expert panel’s judgment using the Lawshe formula. The results showed that all items obtained CVR values above the minimum acceptable threshold, indicating satisfactory content validity. These findings confirm that the items appropriately represent the intended construct and are considered essential by subject matter experts (Table 8).
Discussion
The current study was conducted to develop, validate, and standardize a questionnaire for empty nest syndrome among the elderly. Given that the occurrence of this syndrome during middle age and later years can have a significant social impact on this demographic, the study is of special importance for elucidating the condition and its precise assessment in society. In comparison to other tools designed to measure empty nest syndrome, the tool developed by Mobiz and Equando can be mentioned. This questionnaire is composed of three sections. The first section includes demographic information of the samples such as number of children, marital status, gender, and age. The second section, which contains 16 items, addresses feelings related to empty nest syndrome, and the final section focuses on parental adaptation patterns with 13 items. Moreover, the Cronbach α of the tool developed in the current study aligns with that of the aforementioned questionnaire (0.81) [15].
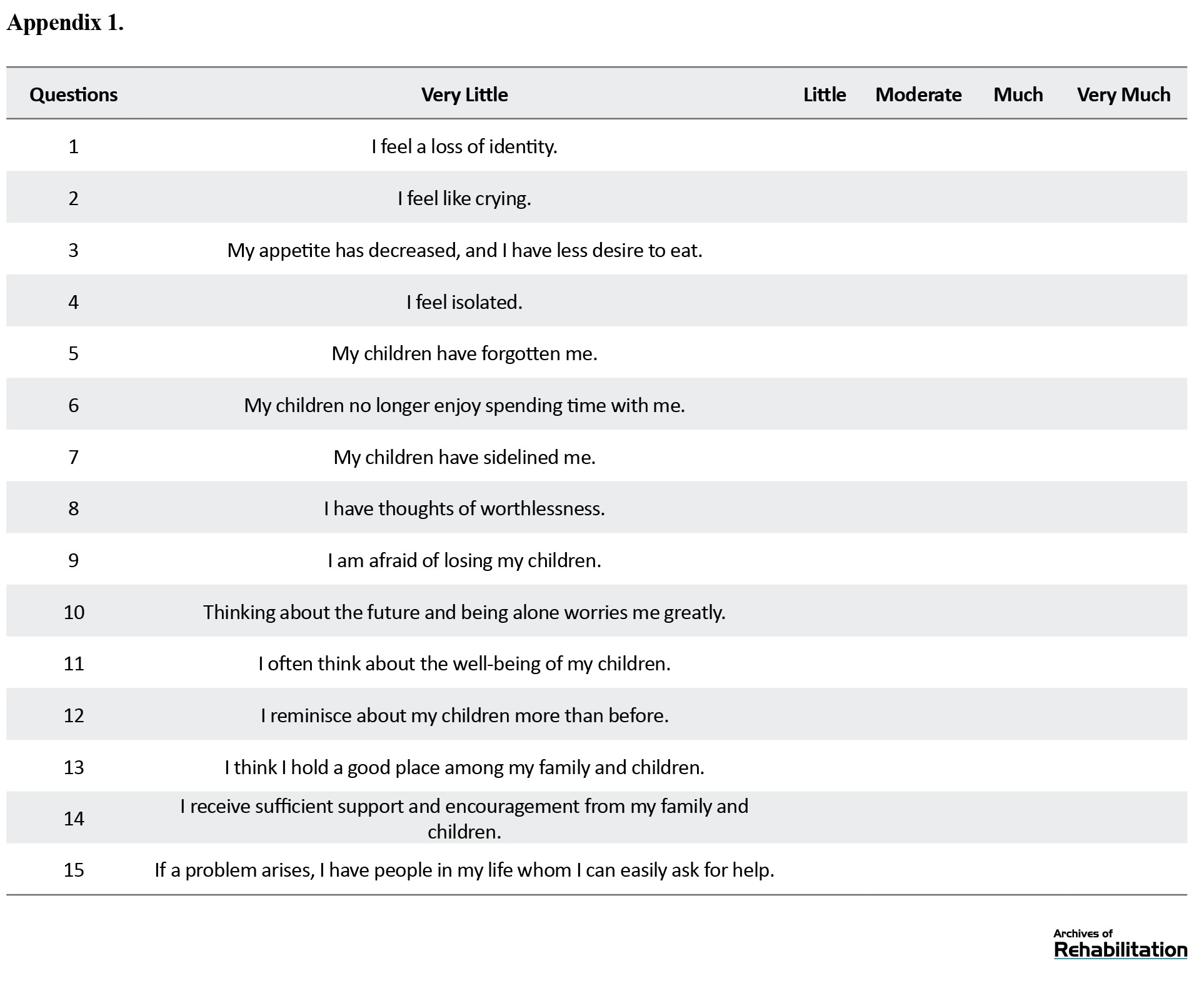
One of the subscales identified in the researcher-developed empty nest syndrome questionnaire is related to the signs of feeling rejected by parents, which includes 8 items (Appendix 1).
The studies by Seiffe-Krenke (2006) demonstrated that when a child leaves home, it is a significant event for both the child and the parents, creating a conflicting time: A period of loving and letting go, and a time when the parental role is gradually relinquished. As children leave home, parents experience a sense of loss, sorrow, and grief that can lead to feelings of depression, possibly exacerbated by worries about the future and increased feelings of loneliness. According to the results of the current study, the level of education has a significant effect on the likelihood of suffering from empty nest syndrome, with illiterate elderly reporting a higher percentage of severe cases [28].
This finding aligns with the research by Mahdiyar et al. (2014), which showed that parents suffering from empty nest syndrome with lower education levels reported a significant increase in feelings of loneliness compared to before their children left home. Major life transitions such as retirement, menopause, childbirth, etc. inherently cause [10] anxiety in life, and since parents with empty nest syndrome face one of these major transitions (the departure of their children), the appearance of anxiety symptoms become one of the main signs of this syndrome in them, directly linked to their children’s situation, especially losing them. Accordingly, the empty nest syndrome questionnaire includes 6 out of the total 15 questions related to examining the signs of fear of losing children in parents, specifically questions 9, 10, 11, and 12. The subscale of fear of losing children in the empty nest syndrome questionnaire has a Cronbach α of 0.80, which aligns with the study by Márquez-González et al., who reported an alpha of 0.91 [29].
Other tools such as the adaptation and validation of the Portuguese version of the elderly anxiety questionnaire by Ribeiro et al. showed a high internal consistency with a Cronbach α of 0.96, which is consistent with the researcher-developed questionnaire [30]. The reduction in receiving social support during old age can impact the level of life satisfaction of the elderly and weaken their social bonds, a phenomenon that is observable in seniors suffering from empty nest syndrome. In the empty nest syndrome questionnaire, 3 questions are specifically designed to assess the concept of social support, namely 13, 14, and 15.
Nabavi et al. (2014) also showed in their studies that increasing social support for the elderly can have a significant impact on their mental health and social functioning [31]. Bavozin and Sepahvandi also demonstrated that the more social support the elderly receive, the more they benefit from social and psychological health [32]. Moreover, the Cronbach α for the social support subscale of life in the empty nest syndrome questionnaire is 0.83, which aligns with the multidimensional social support tool by Zimet et al. with a Cronbach α of 0.83 [33].
Conclusion
One of the main challenges for researchers in the field of gerontology in studying empty nest syndrome is the lack of appropriate tools developed within the Iranian cultural context to measure this phenomenon. Many experts in this field believe that due to cultural relativity, differences, and distinct roots, there is a need for tools with unique features and sensitivities. However, many studies conducted in Iran have merely relied on the presence of parents in the empty nest situation or interviews, which can compromise the results of the studies since merely being alone at home and the departure of children from the home does not necessarily indicate that the parents are suffering from empty nest syndrome. In some cases, parents may feel more satisfied than when their children were at home, which could be due to reduced parental role pressure, spending more leisure time with their spouse, friends, etc.
This study attempted to develop the empty nest syndrome questionnaire using Persian and English theoretical sources, the social and cultural structures of the country, and interviews with experts in gerontology. The measure created in this study was designed considering the social and cultural characteristics of Iranian parents and has been tested, and as the results indicate, the developed tool has suitable validity and reliability. Therefore, this tool can be used as a means to measure empty nest syndrome for researchers in this field.
Study limitations
Every research faces scientific and executive difficulties, and this study is no exception. Considering the theoretical texts, empty nest syndrome shows more manifestation in the first two years after the children’s departure, and in the following years, we will witness the parents’ adaptation to this situation. However, due to the difficulty in collecting samples and coinciding with the COVID-19 pandemic period, we had to involve parents in the research who had a maximum of three years since their children’s departure. In this study, due to time constraints, separate samples were not used for factor analysis and validity and reliability estimation. Given the COVID-19 pandemic and the unavailability of subjects, the time reliability was tested with a sample of 30 people.
Future research suggestions
This measure was specifically created for assessing empty nest syndrome among the elderly and has been evaluated in Tehran. It is recommended that the results of the tool implementation be examined in other cities of the country and for the middle-aged population. Given the results of the study and considering the face, content, construct, and structural validity and reliability of the questionnaire, its use in descriptive studies in gerontology is recommended.
Ethical Considerations
Compliance with ethical guidelines
This research was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1401.119). All ethical principles in this research were observed, and participants were allowed to withdraw from the research at any time. Also, all participants were informed about the research process, and their information was kept confidential.
Funding
This research did not receive any financial support from funding organizations in various sectors. The present article is derived from the master's thesis of Fatemeh Khashaman, approved by the Department of Counseling, School of Rehabilitation Sciences,University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Authors' contributions
Conceptualization, project management, and supervision: Bahman Bahmani and Gholamreza Ghaedamini Harouni; Methodology, validation, and visualization: Fatemeh Khashaman and Gholamreza Ghaedamini; Study design, resources, execution, and writing the original draft: Fatemeh Khashaman; Review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their sincere gratitude to the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran for providing the necessary support and resources for conducting this research.
Test re-test reliability (temporal stability)
To examine the test ret-est reliability (temporal stability), scores from the questionnaire were correlated across two sessions conducted one week apart with 30 subjects. The results of the study indicated a stability index of 0.994, demonstrating the high reliability of the test. Exploratory factor analysis and reliability assessment of the tool were performed using SPSS software, version 26, and confirmatory factor analysis was conducted using Amos software version 24. This questionnaire consists of 15 questions with a 5-point Likert scale ranging from very low to very high. The tool contains three subscales measuring aspects such as feelings of rejection, fear of losing children, and social support for the elderly. Theoretically, this measure evaluates mild to severe symptoms and feelings of empty nest syndrome. Specifically, the total score of the questionnaire is the sum of the scores in each of the three subscales, resulting in a final score ranging from 1 to 95. Scores ranging from 1 to 33 indicate mild empty nest syndrome, scores from 33.1 to 55 suggest moderate syndrome, and scores from 55.1 to 75 indicate high levels of empty nest syndrome.To evaluate the content validity of the questionnaire, the content validity ratio (CVR) was calculated for each item based on the expert panel’s judgment using the Lawshe formula. The results showed that all items obtained CVR values above the minimum acceptable threshold, indicating satisfactory content validity. These findings confirm that the items appropriately represent the intended construct and are considered essential by subject matter experts (Table 8).
Discussion
The current study was conducted to develop, validate, and standardize a questionnaire for empty nest syndrome among the elderly. Given that the occurrence of this syndrome during middle age and later years can have a significant social impact on this demographic, the study is of special importance for elucidating the condition and its precise assessment in society. In comparison to other tools designed to measure empty nest syndrome, the tool developed by Mobiz and Equando can be mentioned. This questionnaire is composed of three sections. The first section includes demographic information of the samples such as number of children, marital status, gender, and age. The second section, which contains 16 items, addresses feelings related to empty nest syndrome, and the final section focuses on parental adaptation patterns with 13 items. Moreover, the Cronbach α of the tool developed in the current study aligns with that of the aforementioned questionnaire (0.81) [15].
One of the subscales identified in the researcher-developed empty nest syndrome questionnaire is related to the signs of feeling rejected by parents, which includes 8 items (Appendix 1).
The studies by Seiffe-Krenke (2006) demonstrated that when a child leaves home, it is a significant event for both the child and the parents, creating a conflicting time: A period of loving and letting go, and a time when the parental role is gradually relinquished. As children leave home, parents experience a sense of loss, sorrow, and grief that can lead to feelings of depression, possibly exacerbated by worries about the future and increased feelings of loneliness. According to the results of the current study, the level of education has a significant effect on the likelihood of suffering from empty nest syndrome, with illiterate elderly reporting a higher percentage of severe cases [28].
This finding aligns with the research by Mahdiyar et al. (2014), which showed that parents suffering from empty nest syndrome with lower education levels reported a significant increase in feelings of loneliness compared to before their children left home. Major life transitions such as retirement, menopause, childbirth, etc. inherently cause [10] anxiety in life, and since parents with empty nest syndrome face one of these major transitions (the departure of their children), the appearance of anxiety symptoms become one of the main signs of this syndrome in them, directly linked to their children’s situation, especially losing them. Accordingly, the empty nest syndrome questionnaire includes 6 out of the total 15 questions related to examining the signs of fear of losing children in parents, specifically questions 9, 10, 11, and 12. The subscale of fear of losing children in the empty nest syndrome questionnaire has a Cronbach α of 0.80, which aligns with the study by Márquez-González et al., who reported an alpha of 0.91 [29].
Other tools such as the adaptation and validation of the Portuguese version of the elderly anxiety questionnaire by Ribeiro et al. showed a high internal consistency with a Cronbach α of 0.96, which is consistent with the researcher-developed questionnaire [30]. The reduction in receiving social support during old age can impact the level of life satisfaction of the elderly and weaken their social bonds, a phenomenon that is observable in seniors suffering from empty nest syndrome. In the empty nest syndrome questionnaire, 3 questions are specifically designed to assess the concept of social support, namely 13, 14, and 15.
Nabavi et al. (2014) also showed in their studies that increasing social support for the elderly can have a significant impact on their mental health and social functioning [31]. Bavozin and Sepahvandi also demonstrated that the more social support the elderly receive, the more they benefit from social and psychological health [32]. Moreover, the Cronbach α for the social support subscale of life in the empty nest syndrome questionnaire is 0.83, which aligns with the multidimensional social support tool by Zimet et al. with a Cronbach α of 0.83 [33].
Conclusion
One of the main challenges for researchers in the field of gerontology in studying empty nest syndrome is the lack of appropriate tools developed within the Iranian cultural context to measure this phenomenon. Many experts in this field believe that due to cultural relativity, differences, and distinct roots, there is a need for tools with unique features and sensitivities. However, many studies conducted in Iran have merely relied on the presence of parents in the empty nest situation or interviews, which can compromise the results of the studies since merely being alone at home and the departure of children from the home does not necessarily indicate that the parents are suffering from empty nest syndrome. In some cases, parents may feel more satisfied than when their children were at home, which could be due to reduced parental role pressure, spending more leisure time with their spouse, friends, etc.
This study attempted to develop the empty nest syndrome questionnaire using Persian and English theoretical sources, the social and cultural structures of the country, and interviews with experts in gerontology. The measure created in this study was designed considering the social and cultural characteristics of Iranian parents and has been tested, and as the results indicate, the developed tool has suitable validity and reliability. Therefore, this tool can be used as a means to measure empty nest syndrome for researchers in this field.
Study limitations
Every research faces scientific and executive difficulties, and this study is no exception. Considering the theoretical texts, empty nest syndrome shows more manifestation in the first two years after the children’s departure, and in the following years, we will witness the parents’ adaptation to this situation. However, due to the difficulty in collecting samples and coinciding with the COVID-19 pandemic period, we had to involve parents in the research who had a maximum of three years since their children’s departure. In this study, due to time constraints, separate samples were not used for factor analysis and validity and reliability estimation. Given the COVID-19 pandemic and the unavailability of subjects, the time reliability was tested with a sample of 30 people.
Future research suggestions
This measure was specifically created for assessing empty nest syndrome among the elderly and has been evaluated in Tehran. It is recommended that the results of the tool implementation be examined in other cities of the country and for the middle-aged population. Given the results of the study and considering the face, content, construct, and structural validity and reliability of the questionnaire, its use in descriptive studies in gerontology is recommended.
Ethical Considerations
Compliance with ethical guidelines
This research was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1401.119). All ethical principles in this research were observed, and participants were allowed to withdraw from the research at any time. Also, all participants were informed about the research process, and their information was kept confidential.
Funding
This research did not receive any financial support from funding organizations in various sectors. The present article is derived from the master's thesis of Fatemeh Khashaman, approved by the Department of Counseling, School of Rehabilitation Sciences,University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Authors' contributions
Conceptualization, project management, and supervision: Bahman Bahmani and Gholamreza Ghaedamini Harouni; Methodology, validation, and visualization: Fatemeh Khashaman and Gholamreza Ghaedamini; Study design, resources, execution, and writing the original draft: Fatemeh Khashaman; Review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their sincere gratitude to the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran for providing the necessary support and resources for conducting this research.
References
- Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020; 139:6-11. [DOI:10.1016/j.maturitas.2020.05.018] [PMID]
- Nouri A, Farsi S. [Expectations of institutionalized elderly from their children (Persian)]. Iranian Journal of Ageing. 2018; 13(2):262-79. [DOI:10.32598/sija.13.2.262]
- Tahan M, Askari Z, Ahangri E. The effectiveness of group therapy based on commitment and acceptance of the increase in life satisfaction in people with empty nest syndrome. Journal of Psychology and Cognition. 2017; 2(3):186-191. [DOI:10.35841/psychology-cognition.2.3.186-187]
- Bougea A, Despoti A, Vasilopoulos E. Empty-nest-related psychosocial stress: Conceptual issues, future directions in economic crisis. Psychiatriki. 2019; 30(4):329-38. [DOI:10.22365/jpsych.2019.304.329] [PMID]
- Mansoor A, Hasan SS. Empty nest syndrome and psychological wellbeing among middle aged adults. Pakistan Journal of Social and Clinical Psychology. 2019; 17(1):55-60. [Link]
- Montajabian Z, Rezai S. [The effectiveness of Meta Cognitive Interpersonal Therapy on Reduction of Perceived pain and Marital Conflict among Couples at Empty Nest Stage (Persian)]. 2021; 12(3):91-103. [Link]
- Parpaee R, Kakaberaei K. [The effectiveness of logotherapy on decreasing depression and anxiety in the elderly women with Empty Nest Syndrome (Persian)]. Aging Psychology. 2018; 4(1):51-9. [Link]
- Young C. Empty Nest Syndrome and parent engagement in activities following the last adult child leaving home: A multiple case study [PhD dissertation)]. Florida: Keiser University; 2021. [Link]
- Chattopadhyay S, Das R. Statistical Validation of LENS: A Smartphone-based Empty Nest Syndrome Screening and Monitoring Biomarker Tool. Indian Journal of Mental Health. 2022; 9(1):71-86. [DOI:10.30877/IJMH.9.1.2022.71-86]
- Mahdiyar F, Khayyer M, Hosseini SM. Comparison between empty nest syndrome in parents, before and after their child (ren) left home. Knowledge & Research in Applied Psychology. 2017; 15(58):17-29. [Link]
- Chen D, Yang X, Aagard SD. The empty nest syndrome: Ways to enhance quality of life. Educational Gerontology. 2012; 38(8):520-9. [DOI:10.1080/03601277.2011.595285]
- Silverstein M, Litwak E. A task-specific typology of intergenerational family structure in later life. The Gerontologist. 1993; 33(2):258-64. [DOI:10.1093/geront/33.2.258] [PMID]
- Pargar F, Abolhasane RS. Evaluation of complications associated in empty middle-aged mothers. Entomology and Applied Science Letters. 2020; 7(4-2020):58-65. [Link]
- Wu ZQ, Sun L, Sun YH, Zhang XJ, Tao FB, Cui GH. Correlation between loneliness and social relationship among empty nest elderly in Anhui rural area, China. Aging and Mental Health. 2010; 14(1):108-12. [DOI:10.1080/13607860903228796] [PMID]
- Mbaeze I, Ukwandu E. Empty-nest syndrome, gender and family size as predictors of aged’s adjustment pattern. Pakistan Journal of Social Sciences. 2011; 8(4):166-71. [Link]
- Fountoulakis KN, Siamouli M, Magiria S, Kaprinis G. Late-life depression, religiosity, cerebrovascular disease, cognitive impairment and attitudes towards death in the elderly: Interpreting the data. Medical hypotheses. 2008; 70(3):493-6. [DOI:10.1016/j.mehy.2007.01.093] [PMID]
- Stancliffe RJ, Wiese MY, Read S, Jeltes G, Clayton JM. Knowing, planning for and fearing death: Do adults with intellectual disability and disability staff differ? Research in Developmental Disabilities. 2016; 49-50:47-59. [DOI:10.1016/j.ridd.2015.11.016] [PMID]
- Perlman D. Loneliness: A life-span, family perspective. In: Milardo RM, editoe. Families and Social Networks. California: Sage Publications, Inc. 1988. [Link]
- Jaremka LM, Fagundes CP, Glaser R, Bennett JM, Malarkey WB, Kiecolt-Glaser JK. Loneliness predicts pain, depression, and fatigue: understanding the role of immune dysregulation. Psychoneuroendocrinology. 2013; 38(8):1310-7. [DOI:10.1016/j.psyneuen.2012.11.016] [PMID]
- Kline RB, Santor DA. Principles & practice of structural equation modelling. Canadian Psychology. 1999; 40(4):381-3. [Link]
- Schreiber JB, Nora A, Stage FK, Barlow EA, King J. Reporting structural equation modeling and confirmatory factor analysis results: A review. The Journal of Educational Research. 2006; 99(6):323-38. [DOI:10.3200/JOER.99.6.323-338]
- Gillham B. Research Interview. London: Bloomsbury Publishing; 2001. [Link]
- Lawshe CH. A quantitative approach to content validity. Personnel Psychology. 1975; 28(4):563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
- Keyes CL, Wissing M, Potgieter JP, Temane M, Kruger A, Van Rooy S. Evaluation of the mental health continuum-short form (MHC-SF) in setswana-speaking South Africans. Clinical Psychology & Psychotherapy. 2008; 15(3):181-92. [DOI:10.1002/cpp.572] [PMID]
- Penning MJ, Liu G, Chou PHB. Measuring loneliness among middle-aged and older adults: The UCLA and de Jong Gierveld loneliness scales. Social Indicators Research. 2014; 118:1147-66. [DOI:10.1007/s11205-013-0461-1]
- Hosseinabadi R, Foroughan M, Ghaed Amini Harouni GR, Zeidali Beiranvand R, Pournia Y. [Psychometric properties of the Persian version of the 6-item De Jong Gierveld loneliness scale in Iranian community-dwelling older persons (Persian)]. Salmand: Iranian Journal of Ageing. 2020; 15(3):338-49. [DOI: 10.32598/sija.15.3.2515.2]
- Mehrabi S, Delavari A, Moradi G, Esmailnasab EN, Pooladi A, Alikhani S, et al. [Smoking among 15-to 64-year-old Iranian people in 2005 (Persian)]. Iranian Journal of Epidemiology. 2007; 3(1):1-9. [Link]
- Seiffe-Krenke I. Leaving home or still in the nest? Parent-child relationships and psychological health as predictors of different leaving home patterns. Developmental Psychology. 2006; 42(5):864-76. [DOI:10.1037/0012-1649.42.5.864] [PMID]
- Márquez-González M, Losada A, Fernández-Fernández V, Pachana NA. Psychometric properties of the Spanish version of the Geriatric Anxiety Inventory. International Psychogeriatrics. 2012; 24(1):137-44. [DOI:10.1017/S1041610211001505] [PMID]
- Ribeiro O, Paúl C, Simões MR, Firmino H. Portuguese version of the Geriatric Anxiety Inventory: Transcultural adaptation and psychometric validation. Aging & Mental Health. 2011; 15(6):742-8. [DOI:10.1080/13607863.2011.562177] [PMID]
- Nabavi SH, Alipour F, Hejazi A, Rabani E, Rashedi V. [Relationship between social support and mental health in older adults (Persian)]. Medical Journal of Mashhad University of Medical Sciences. 2014; 57(7):841-6. [DOI:10.22038/mjms.2014.3756]
- Bavazin F, Sepahvandi M. [The study of the relationship between social support and social and psychological well-being among elderly people in city of Khorramabad in 2017 (Persian)]. Nursing and Midwifery Journal. 2018; 15(12):931-8. [Link]
- Besharat MA. [Multidimensional Scale of Perceived Social Support: Questionnaire, Instruction and Scoring (Persian)]. Developmental Psychology (Journal of Iranian Psychologists). 2019; 15(60):336-8. [Link]
Type of Study: Applicable |
Subject:
General Psychology
Received: 23/09/2023 | Accepted: 24/09/2024 | Published: 1/04/2025
Received: 23/09/2023 | Accepted: 24/09/2024 | Published: 1/04/2025
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
