

Volume 23, Issue 4 (Winter 2023)
jrehab 2023, 23(4): 518-539 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Faraji M, Haghgoo H A, Peshyareh E, Monfared E, Vahedi M. Investigating the Correlation Between Computer Tests (CANTAB) and Functional Cognitive Tests (LOTCA) With the Participation of People With Multiple Sclerosis in Daily Life Activities. jrehab 2023; 23 (4) :518-539
URL: http://rehabilitationj.uswr.ac.ir/article-1-2982-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-2982-en.html



1- Department of Occupational Therapy, Faculty of Rehabilitation Sciences, University of Rehabilitation Sciences and Social Health, Tehran, Iran., Department of Occupational Therapy, School of Rehabilitation, University of Social Welfare and Rehabilitation, Tehran, Iran
2- Department of Occupational Therapy, Faculty of Rehabilitation Sciences, University of Rehabilitation Sciences and Social Health, Tehran, Iran. ,h.haghgoo@yahoo.com
3- Department of Biostatistics and Epidemiology, Faculty of Rehabilitation Sciences, University of Rehabilitation Sciences and Social Health, Tehran, Iran., Department of Biostatistics and Epidemiology, School of Rehabilitation, University of Social Welfare and Rehabilitation, Tehran, Iran
2- Department of Occupational Therapy, Faculty of Rehabilitation Sciences, University of Rehabilitation Sciences and Social Health, Tehran, Iran. ,
3- Department of Biostatistics and Epidemiology, Faculty of Rehabilitation Sciences, University of Rehabilitation Sciences and Social Health, Tehran, Iran., Department of Biostatistics and Epidemiology, School of Rehabilitation, University of Social Welfare and Rehabilitation, Tehran, Iran
Keywords: Multiple sclerosis, Community integration questionnaire, Lowenstein occupational therapy cognitive assessment (LOTCA), Cambridge neuropsychological test automated battery (CANTAB)
Full-Text [PDF 2526 kb]
(1677 Downloads)
| Abstract (HTML) (3533 Views)
Full-Text: (1687 Views)
Introduction
Multiple sclerosis (MS) is a progressive disease of the central nervous system characterized by diffuse lesions or plaques in the brain and spinal cord that causes problems in cognitive function [1]. Cognition is a mental activity or the process of acquiring knowledge and understanding through thinking, experience, and senses [2]. This activity is disturbed in people with central nervous system involvement. As a result, cognitive disorders affect the performance of people with MS [3]. Considering the impact of cognitive function on the life process of a person, the need for rehabilitation in people with MS is important.
Rehabilitation is a process through which participation and individual and environmental interactions can create adaptation. In other words, rehabilitation consists of appropriate measures to empower people with disabilities to achieve and maintain their maximum physical, mental, and social independence and full participation in all aspects of life [4]. Getting the person to participate in daily activities is the basis of the rehabilitation process and its goal. For this reason, it is very important to determine a person’s level of participation in daily living activities [5].
In 2001, the World Health Organization (WHO) defined the concept of participation as “Involvement in life situations” in the sense that a person participates in daily life situations [6]. There are semi-structured and structured interviews that along with other tools provide therapists with information that estimates a person’s participation. In occupational therapy, there are many tools and devices, among which we can mention functional and computer tools, used to predict and plan the rehabilitation process [7].
In people with MS, cognitive disorders have a direct and great impact on their performance in daily living activities. Aronson stated that MS greatly impacts people’s performance and quality of everyday life, and one of the destructive consequences of this disorder is job loss in 24% to 80% of these patients [8]. Therefore, examining cognitive domains can help us in clinical decision-making and interventions. Another positive result is earlier access to the relationship between cognitive impairment and the level of participation.
If the relationship between cognitive impairment and participation is not determined well, a complete assessment cannot be obtained, especially in matters related to daily living activities. Another consequence is that an effective treatment plan that covers the impact of cognitive impairment on participation is not created. Since improving people’s quality of life is important and necessary, the researchers should find a tool that has a better and greater relationship with the level of individual participation. This tool provides us with reliable, practical, complete, and quick results to realize the individual’s independence [9].
Computer and functional tools are used to assess the cognitive disorders of people with MS. For this reason, measuring these tools’ correlation with people’s level of participation can be a great step towards improving the quality of rehabilitation services and quality of life of these people. In various studies, two computer and functional tools have been examined and compared. Among them, we can mention the loss of flexibility in computer tests, the computer skills of people, and the high accuracy of computer scores. For example, the time-consuming performance tools have been discussed.
Considering all these things, this research aims to investigate the relationship between computer participation and functional tools so that the best decision can be made in clinical matters according to different conditions. Considering the impact of this disease on the individual’s performance, it is important and necessary to find the answer to which of these tools is a better representative or predictor to determine the level of participation.
Materials and Methods
The current research is cross-sectional and of the correlational type.
Statistical population
The study population comprised patients with MS admitted to Hazrat Abolfazl Rehabilitation Clinic and MS Center of Isfahan City, Iran, who met the inclusion criteria in the winter of 2020. The inclusion criteria included a willingness to participate in the research, a definite diagnosis of MS by a specialist doctor, having an expanded disability status scale (EDSS) scale score of 1 to 5 (diagnosed by a neurologist), lacking mental problems and fractures, ability to work with a computer, not taking corticosteroids for 28 days before the test [10, 11], lacking a history of other neurological diseases, not being addicted, ability to give informed consent. The exclusion criteria included not completing the tests and recurrence of attacks while completing the tests.
Initially, a pilot study was conducted on 15 people due to the lack of a similar study. According to the data analysis, the studied sample was 45 MS patients (36 women and 9 men) aged 19 to 69 years. Available non-probability sampling (true experimental) was used. The way to choose people was available probability sampling. In this study, based on the participant’s inclusion criteria, they were placed in one of the two groups by randomly choosing from among two pieces of paper on which their group name was written, one of which was an even and the other was an odd one.
If the examiner randomly chooses the paper containing the odd number, the patient will be placed in the odd group. In the first session, the patient would do the cambridge neuropsychological test automated battery (CANTAB) test, and in the second session, the patient would do the loewenstein occupational therapy cognitive assessment (LOTCA) test and answer the community integration questionnaire. If the examiner chose a paper that contained an even number, the patient would do the LOTCA test and answer the community integration questionnaire in the first session and do the CANTAB test in the second session.
Data collection tools
Data collection was done between 9:00 AM and 12:00 PM to avoid the effects of fatigue on the results. There were four instruments for data collection:
Questionnaire: It is a questionnaire to collect data on participants’ age, sex, education level, employment status, marital status, family history, type of MS, EDSS score, and history of other mental or physical disorders.
LOTCA Test: It is a set of tests designed for occupational therapists to evaluate a person’s cognitive processes and determine how well a person can perform daily functional tasks.
CANTAB Test: It is a set of computer neuropsychological tests developed at Cambridge University and used to evaluate cognitive components [12]. In this research, we used 3 tests, spatial span test (SST), stockings of Cambridge (SOC), and delayed matching to sample (DMS) from the set of CANTAB tests.
DMS Test: This test evaluates the simultaneous visual matching ability and short-term visual recognition memory for non-verbal patterns [13].
SOC Test: It is related to spatial planning, which forces people to use problem-solving strategies and match and visual perception of two sets of stimuli.
SST Test: The test evaluates working memory and short-term memory [14].
Community Integration Questionnaire: This questionnaire was designed to evaluate the level of participation in home integration, social integration, and purposeful and productivity integration activities in people with brain damage [21].
In this research, three areas of the integration questionnaire, including home integration, social integration, and purposeful activities integration, were measured with the sub-tests of CANTAB and LOTKA’s cognitive test. The scores of each test were obtained. The statistical data were analyzed with SPSS software.
Results
According to the information obtained from the people through the demographic questionnaire, the average, the mean and standard deviation, and the minimum and maximum values of indicators are given for the quantitative variables. For qualitative variables, their frequency and percentage are reported. Information about the participants is provided in the following tables.
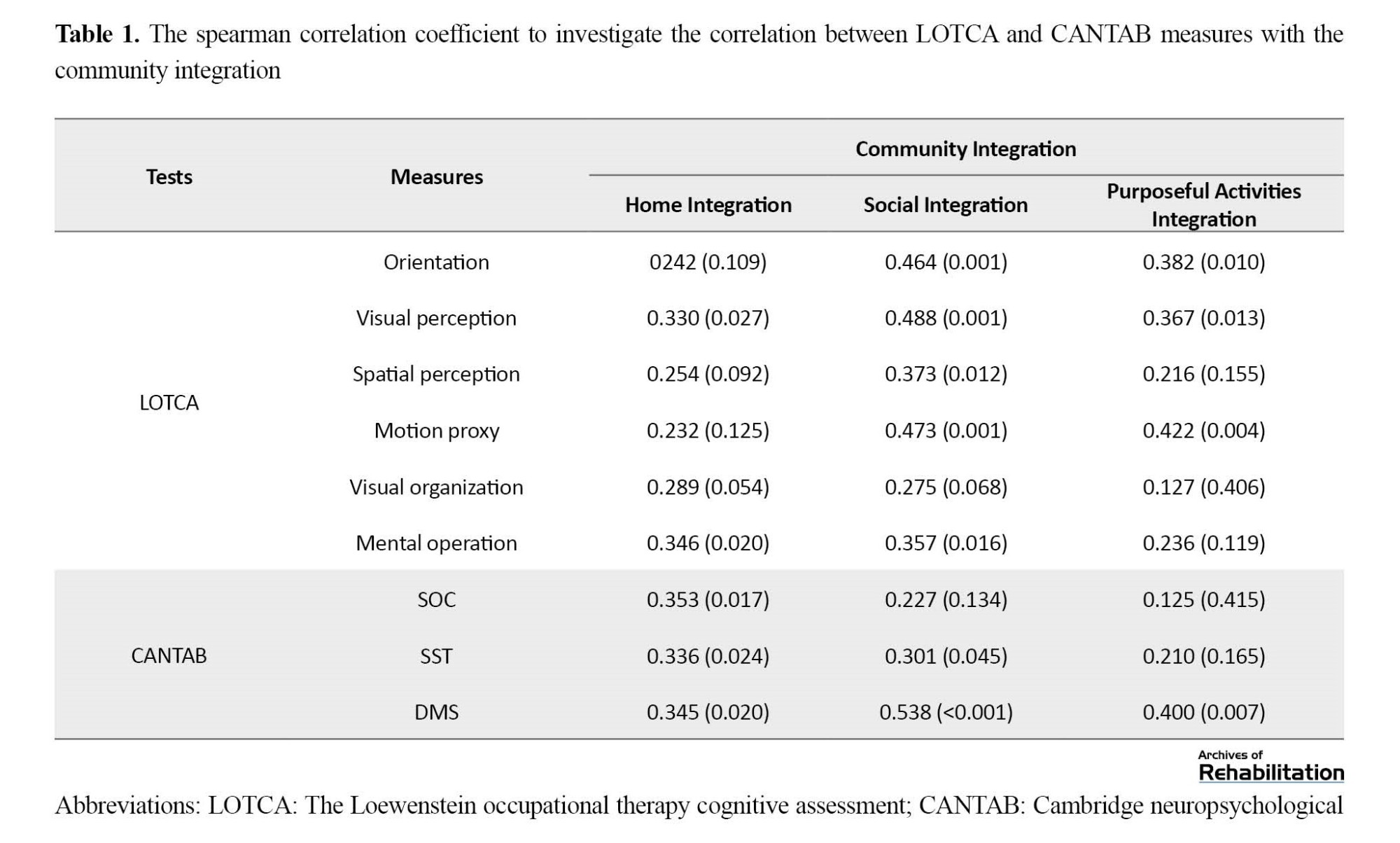
Due to the non-establishment of the normality assumption for most of these measures, the Spearman correlation coefficient should be used. The significance level of the non-linear relationship between the two measurements is 0.05. Table 1 presents the results of the Spearman correlation coefficient. The correlation coefficient value is given in the first row for each house in the Table. The probability value related to the linear correlation test of two variables is provided in the second row (the number in parentheses).
The required tests in this research
The DMS test is primarily sensitive to damage in the medial temporal lobe area and then with some input from the frontal lobes. This test evaluates simultaneous visual matching ability and short-term visual recognition memory for non-verbal patterns. In the DMS test, 14 criteria can be divided into 3 groups: response delay, the number and percentage of correct and incorrect responses, and theoretical measures in response detection directions [13].
This study chose the number and percentage of correct and incorrect answers as the change criteria. The higher the number of correct answers in the test, the higher the percentage score. A higher score indicates better performance [14].
The SOC test is related to spatial planning, which forces people to use problem-solving strategies and match and visual perception of two sets of stimuli. Also, this test evaluates working memory and shows the frontal lobe’s function. In the SOC test, there are 4 change criteria, which include the ability to solve the problem in the fewest moves, the average of 2, 3, 4, and 5 moves to solve the problem, the amount of thinking time to solve problems with 2, 3, 4, and 5 moves, additional thinking time to solve problems with 2, 3, 4 and 5 moves [13].
In this study, the score obtained from the ability to solve the problem in the least movement was chosen as the criterion of change. The higher the number of correct answers in the smallest movement, the higher the score on the test. A higher score indicates better problem-solving ability and better performance [14].
The SST test evaluates working memory and short-term memory, an assessment of frontal lobe function. In the SST test, 6 measures can be grouped into 4 categories: number of correct answers, errors, number of attempts, and delay [13]. In this study, the score obtained from the number of correct answers was chosen as the change criterion. The higher the number of correct answers, the higher the score. A higher score indicates a person’s better performance [14].
Community integration questionnaire
This questionnaire is designed to evaluate the level of participation in home integration, social integration, and purposeful and productivity integration activities in people with brain damage. This tool includes 15 items completed by the person himself, the caregiver, or a family member [1, 15]. This tool has also been used for patients with spinal cord injuries, orthopedic injuries, and MS. This tool can be used in the evaluation process, during the intervention, and during the follow-up after the intervention. The validity and reliability of the community integration questionnaire were conducted in 2012 by Negahban et al. in Iran with 105 MS patients [16]. This questionnaire includes the following items:
1. Home integration: It includes 5 items that show the degree of independence of a person in performing daily activities.
2. Social integration: It includes 6 items that show the person’s social activity level in the last month.
3. Purposeful activities integration: It includes 4 items that measure productive activities.
The total score of 15 questions ranges from 0 to 29, where the maximum score corresponds to the highest level of integration, and the minimum score corresponds to the lowest level of integration. The score of each question is from 0 to 2. Score 2 indicates maximum integrity in the relevant question, which is how most questions are scored, except for the last 3 questions, which are scored together and range from 0 to 5 [17].
According to Table 2, all the correlations between the LOTCA and CANTAB tests with the community integration were positive, so with the increase in the score of one measure, another measure also increases. The measure of home integration had the most significant linear relationship with the measures of LOTCA’s mental operation and visual perception, respectively. Also, a significant correlation was seen with all three measures of the CANTAB test.

Social integration had a significant positive relationship with all LOTCA measures except visual organization and all CANTAB measures except SOC. Purposeful activities integration also had a significant linear relationship with orientation, visual perception, and motion proxy from LOTCA’s test and only with DMS from CANTAB’s test. In general, there is a correlation between these two tests of community integration, and this test can be used, but this connection is moderate and not strong.
Table 3 presents the intensity and direction of the relationship between CANTAB and LOTCA measures and its prediction by the community integration test measures with the help of linear regression.
According to Table 3, the measure of home integration has a positive significant relationship with all measures of LOTCA and CANTAB. Still, this relationship is significant only with measures of the visual organization of LOTCA and DMS. For example, for one unit increase in the home integration score, on average, the DMS score increases by 1.320 units. In other words, the coefficient of home integration can be equivalent to the measure of the visual organization from LOTCA’s test and DMS from CANTAB’s test.

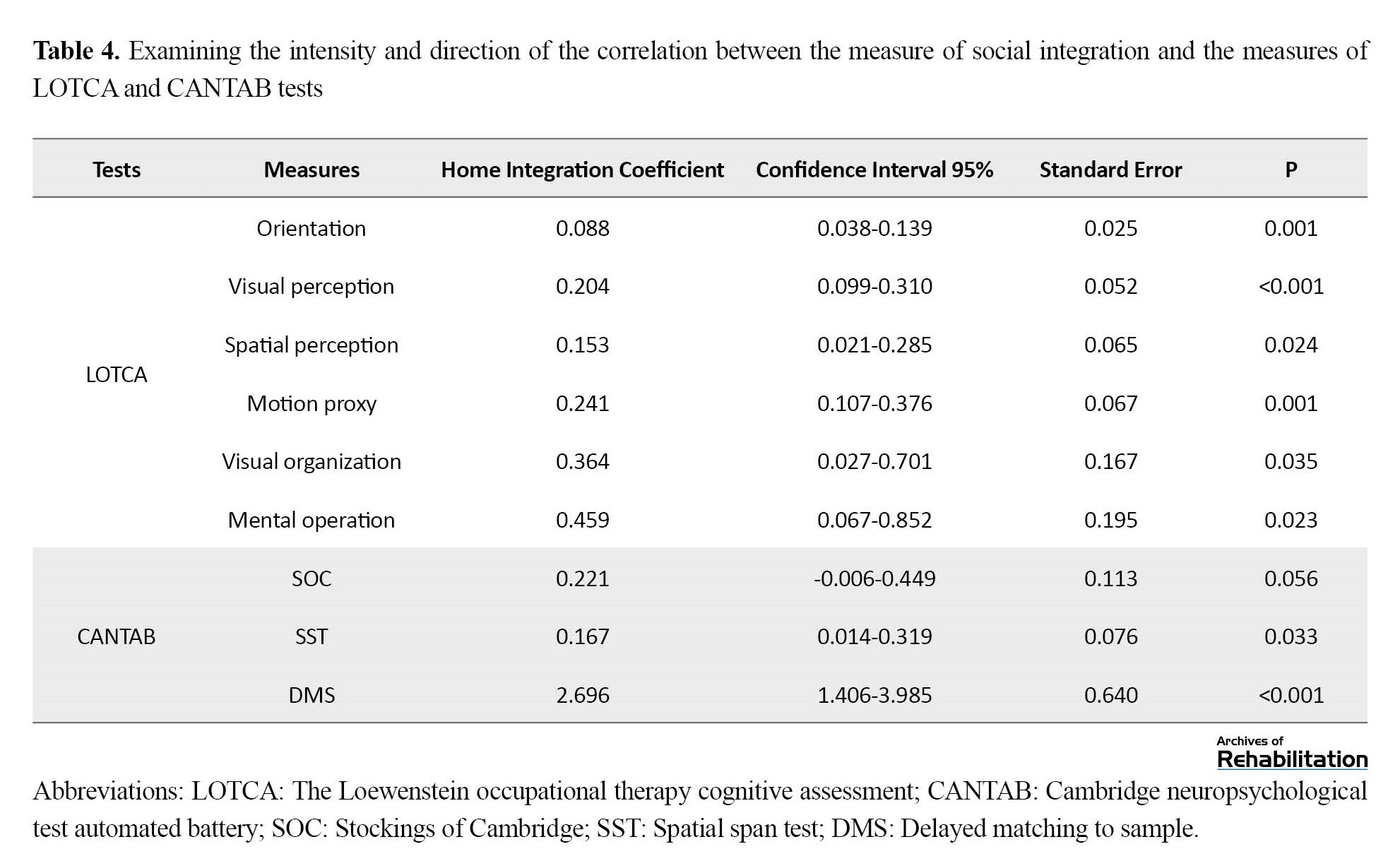
Table 4 presents the results of examining the intensity and direction of the correlation of the social integration measure with all LOTCA and CANTAB measures. All these relationships were positive, and all measures except SOC had significant relationships.
Based on the investigation of the intensity and the direction of the correlation of the measures, Table 5 presents the purposeful activities integration with all measures of LOTCA and CANTAB. This measure had a significant relationship with orientation, visual perception, and motion proxy from LOTCA’s test and DMS from CANTAB’s test.

Discussion
Regarding the impact of MS on participation, Aronson stated that MS greatly impacts people’s function and quality of daily life. He stated that one of the destructive consequences of this disorder is job loss of 24% to 80% of these patients [8].
Also, Taylor et al. compared the functional and computer tests in a review of the articles of the last 15 years. At first, they reviewed the primary research on this topic. Based on these research studies, they stated that the initial research on comparing computer and functional tests mainly tended towards functional tests due to better performance, accuracy, and participation. In the end, they stated that due to the dispersion of research, it is very difficult to express the correlation between these two tests and suggested more practical investigations [18].
Lashpin, in defense of computer tests, dealt with evaluating the cognitive functions of MS patients. He stated that because traditional methods, such as using functional tests to evaluate patients, are time-consuming and difficult to obtain, it is better to use computer versions of the tests [19]. In another study, Scherer researched several functional tests to measure cognitive functions in patients with MS. He stated that since time and cost savings are always important, the best cognitive test should be chosen for each of the problems of MS patients [20].
Willer B et al. used the community integration questionnaire to investigate the participation status of people with traumatic brain injury after rehabilitation in New York City. The study shows that this test is a good indicator of the participation of people who have received rehabilitation services rather than those who have not received them [21].
Based on our research, which was designed to measure the relationship between two types of computer and functional tests with the participation rate in people with MS, these patients were selected according to the required criteria. For this purpose, the valid and standard computer test CANTAB was used as a computer tool, and the valid and standard LOTCA test was used as a functional tool to investigate the cognitive function in people with MS. Also, the community integration questionnaire was used to check the level of participation of people with MS in daily life.
People were given information about how to complete the tests and the questionnaire. Subsequently, people were randomly classified into odd and even groups to avoid tiredness, and the tests and the questionnaire completion were done two times. After performing the tests, the data were collected and analyzed.
The results indicate a relative and appropriate relationship between the participation questionnaire and both types of computer tests of CANTAB and functional tests of LOTCA. According to the results, the community integration questionnaire showed a greater relationship with the CANTAB computer test than with the LOTCA functional test. By realizing this result, therapists can use computer tests instead of functional tests.
The results of the reviews
Home integration shows the greatest convergence with the SOC test in CANTAB. The SOC test is related to spatial planning, which forces people to use problem-solving strategies and match and visual perception of two sets of stimuli. Also, this test evaluates working memory and shows the frontal lobe’s function [14]. So, according to the results, the SOC test measures the factors considered in home integration better. After SOC, it has the highest convergence with mental operations from the LOTCA test, DMS, and SST from the CANTAB test.
Social integration has the highest convergence with DMS from the CANTAB test. The DMS test evaluates the ability to adapt vision and short-term memory and is sensitive to medial and frontal temporal lobe inputs [14]. Therefore, according to the results, the DMS test is more suitable for evaluating the desired factors in social integration. After DMS, it has the highest convergence with visual perception, motion proxy, and orientation from the LOTCA test.
Purposeful activities integration has the greatest convergence with motion proxy from the LOTCA test. Motion proxy assesses a person’s ability to imitate movement actions, use objects, and perform symbolic actions. Therefore, according to the results, the motion proxy item is better for evaluating the factors considered in purposeful activities integration. Also, purposeful activities integration after motion proxy has the highest convergence with DMS from the CANTAB test and orientation and visual perception from the LOTCA test.
The results obtained from this research can be used to advance previous studies. According to the results of this research, which show a high convergence between two computer and functional tests with the participation rate, the use of both tests can be preferred in certain circumstances.
As mentioned, computer tests provide more accurate results [20], and they are cheaper, but they may be stressful and cause more fatigue for the person [23]. As the rate of participation in computer and functional tests is discussed, some researchers stated that the rate of participation is higher in computer tests [22, 24]. Some say that the physical nature of the screen requires more cognitive processes [25] and fewer keyboard skills [26], and the participation of people in functional tests is more than in computer tests.
A very important point in this regard is the way of grading computer and functional tests. Human agents perform functional tests. Many conditions, such as the way people are graded, can affect the score obtained by a person, while in computer tests, human factors are not involved in scoring, and the person gets an accurate score [27].
Conclusion
According to the results of this research, which show a good convergence between two computer and functional tests with the participation rate, it can be said that the use of both tests can be preferred in certain circumstances.
Ethical Considerations
Compliance with ethical guidelines
In the implementation of the research, ethical considerations were considered following the instructions of the Ethics Committee of University of Social Welfare and Rehabilitation Sciences. These principles included obtaining the written consent of the participants, keeping the information confidential, making the participants aware of the research process, not exposing the participants to risk, and promoting human health while maintaining dignity (Code: IR.USWR.REC.2020.215).
Funding
This study was extracted from the first author’s master’s thesis, Department of Occupational Therapy, University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Conceptualization: Hojat Allah Haqgoo, Ebrahim Peshyareh, Milad Faraji, and Elyas Monfared; Methodology, validation, and sources: Mohsen Vahedi and Milad Faraji; Analysis: Hojat Allah Haqgou, Mohsen Vahedi, and Milad Faraji; Research, review and visualization: Milad Faraji and Elyas Monfared; Financing and writing the draft: Milad Faraji; Research management, editing and finalization: Hojat Allah Haqgoo and Milad Faraji; Supervision: Hojat Allah Haqgoo and Ebrahim Peshyareh.
Conflict of interest
The authors declared no conflict of interest.
Multiple sclerosis (MS) is a progressive disease of the central nervous system characterized by diffuse lesions or plaques in the brain and spinal cord that causes problems in cognitive function [1]. Cognition is a mental activity or the process of acquiring knowledge and understanding through thinking, experience, and senses [2]. This activity is disturbed in people with central nervous system involvement. As a result, cognitive disorders affect the performance of people with MS [3]. Considering the impact of cognitive function on the life process of a person, the need for rehabilitation in people with MS is important.
Rehabilitation is a process through which participation and individual and environmental interactions can create adaptation. In other words, rehabilitation consists of appropriate measures to empower people with disabilities to achieve and maintain their maximum physical, mental, and social independence and full participation in all aspects of life [4]. Getting the person to participate in daily activities is the basis of the rehabilitation process and its goal. For this reason, it is very important to determine a person’s level of participation in daily living activities [5].
In 2001, the World Health Organization (WHO) defined the concept of participation as “Involvement in life situations” in the sense that a person participates in daily life situations [6]. There are semi-structured and structured interviews that along with other tools provide therapists with information that estimates a person’s participation. In occupational therapy, there are many tools and devices, among which we can mention functional and computer tools, used to predict and plan the rehabilitation process [7].
In people with MS, cognitive disorders have a direct and great impact on their performance in daily living activities. Aronson stated that MS greatly impacts people’s performance and quality of everyday life, and one of the destructive consequences of this disorder is job loss in 24% to 80% of these patients [8]. Therefore, examining cognitive domains can help us in clinical decision-making and interventions. Another positive result is earlier access to the relationship between cognitive impairment and the level of participation.
If the relationship between cognitive impairment and participation is not determined well, a complete assessment cannot be obtained, especially in matters related to daily living activities. Another consequence is that an effective treatment plan that covers the impact of cognitive impairment on participation is not created. Since improving people’s quality of life is important and necessary, the researchers should find a tool that has a better and greater relationship with the level of individual participation. This tool provides us with reliable, practical, complete, and quick results to realize the individual’s independence [9].
Computer and functional tools are used to assess the cognitive disorders of people with MS. For this reason, measuring these tools’ correlation with people’s level of participation can be a great step towards improving the quality of rehabilitation services and quality of life of these people. In various studies, two computer and functional tools have been examined and compared. Among them, we can mention the loss of flexibility in computer tests, the computer skills of people, and the high accuracy of computer scores. For example, the time-consuming performance tools have been discussed.
Considering all these things, this research aims to investigate the relationship between computer participation and functional tools so that the best decision can be made in clinical matters according to different conditions. Considering the impact of this disease on the individual’s performance, it is important and necessary to find the answer to which of these tools is a better representative or predictor to determine the level of participation.
Materials and Methods
The current research is cross-sectional and of the correlational type.
Statistical population
The study population comprised patients with MS admitted to Hazrat Abolfazl Rehabilitation Clinic and MS Center of Isfahan City, Iran, who met the inclusion criteria in the winter of 2020. The inclusion criteria included a willingness to participate in the research, a definite diagnosis of MS by a specialist doctor, having an expanded disability status scale (EDSS) scale score of 1 to 5 (diagnosed by a neurologist), lacking mental problems and fractures, ability to work with a computer, not taking corticosteroids for 28 days before the test [10, 11], lacking a history of other neurological diseases, not being addicted, ability to give informed consent. The exclusion criteria included not completing the tests and recurrence of attacks while completing the tests.
Initially, a pilot study was conducted on 15 people due to the lack of a similar study. According to the data analysis, the studied sample was 45 MS patients (36 women and 9 men) aged 19 to 69 years. Available non-probability sampling (true experimental) was used. The way to choose people was available probability sampling. In this study, based on the participant’s inclusion criteria, they were placed in one of the two groups by randomly choosing from among two pieces of paper on which their group name was written, one of which was an even and the other was an odd one.
If the examiner randomly chooses the paper containing the odd number, the patient will be placed in the odd group. In the first session, the patient would do the cambridge neuropsychological test automated battery (CANTAB) test, and in the second session, the patient would do the loewenstein occupational therapy cognitive assessment (LOTCA) test and answer the community integration questionnaire. If the examiner chose a paper that contained an even number, the patient would do the LOTCA test and answer the community integration questionnaire in the first session and do the CANTAB test in the second session.
Data collection tools
Data collection was done between 9:00 AM and 12:00 PM to avoid the effects of fatigue on the results. There were four instruments for data collection:
Questionnaire: It is a questionnaire to collect data on participants’ age, sex, education level, employment status, marital status, family history, type of MS, EDSS score, and history of other mental or physical disorders.
LOTCA Test: It is a set of tests designed for occupational therapists to evaluate a person’s cognitive processes and determine how well a person can perform daily functional tasks.
CANTAB Test: It is a set of computer neuropsychological tests developed at Cambridge University and used to evaluate cognitive components [12]. In this research, we used 3 tests, spatial span test (SST), stockings of Cambridge (SOC), and delayed matching to sample (DMS) from the set of CANTAB tests.
DMS Test: This test evaluates the simultaneous visual matching ability and short-term visual recognition memory for non-verbal patterns [13].
SOC Test: It is related to spatial planning, which forces people to use problem-solving strategies and match and visual perception of two sets of stimuli.
SST Test: The test evaluates working memory and short-term memory [14].
Community Integration Questionnaire: This questionnaire was designed to evaluate the level of participation in home integration, social integration, and purposeful and productivity integration activities in people with brain damage [21].
In this research, three areas of the integration questionnaire, including home integration, social integration, and purposeful activities integration, were measured with the sub-tests of CANTAB and LOTKA’s cognitive test. The scores of each test were obtained. The statistical data were analyzed with SPSS software.
Results
According to the information obtained from the people through the demographic questionnaire, the average, the mean and standard deviation, and the minimum and maximum values of indicators are given for the quantitative variables. For qualitative variables, their frequency and percentage are reported. Information about the participants is provided in the following tables.
Due to the non-establishment of the normality assumption for most of these measures, the Spearman correlation coefficient should be used. The significance level of the non-linear relationship between the two measurements is 0.05. Table 1 presents the results of the Spearman correlation coefficient. The correlation coefficient value is given in the first row for each house in the Table. The probability value related to the linear correlation test of two variables is provided in the second row (the number in parentheses).
The required tests in this research
The DMS test is primarily sensitive to damage in the medial temporal lobe area and then with some input from the frontal lobes. This test evaluates simultaneous visual matching ability and short-term visual recognition memory for non-verbal patterns. In the DMS test, 14 criteria can be divided into 3 groups: response delay, the number and percentage of correct and incorrect responses, and theoretical measures in response detection directions [13].
This study chose the number and percentage of correct and incorrect answers as the change criteria. The higher the number of correct answers in the test, the higher the percentage score. A higher score indicates better performance [14].
The SOC test is related to spatial planning, which forces people to use problem-solving strategies and match and visual perception of two sets of stimuli. Also, this test evaluates working memory and shows the frontal lobe’s function. In the SOC test, there are 4 change criteria, which include the ability to solve the problem in the fewest moves, the average of 2, 3, 4, and 5 moves to solve the problem, the amount of thinking time to solve problems with 2, 3, 4, and 5 moves, additional thinking time to solve problems with 2, 3, 4 and 5 moves [13].
In this study, the score obtained from the ability to solve the problem in the least movement was chosen as the criterion of change. The higher the number of correct answers in the smallest movement, the higher the score on the test. A higher score indicates better problem-solving ability and better performance [14].
The SST test evaluates working memory and short-term memory, an assessment of frontal lobe function. In the SST test, 6 measures can be grouped into 4 categories: number of correct answers, errors, number of attempts, and delay [13]. In this study, the score obtained from the number of correct answers was chosen as the change criterion. The higher the number of correct answers, the higher the score. A higher score indicates a person’s better performance [14].
Community integration questionnaire
This questionnaire is designed to evaluate the level of participation in home integration, social integration, and purposeful and productivity integration activities in people with brain damage. This tool includes 15 items completed by the person himself, the caregiver, or a family member [1, 15]. This tool has also been used for patients with spinal cord injuries, orthopedic injuries, and MS. This tool can be used in the evaluation process, during the intervention, and during the follow-up after the intervention. The validity and reliability of the community integration questionnaire were conducted in 2012 by Negahban et al. in Iran with 105 MS patients [16]. This questionnaire includes the following items:
1. Home integration: It includes 5 items that show the degree of independence of a person in performing daily activities.
2. Social integration: It includes 6 items that show the person’s social activity level in the last month.
3. Purposeful activities integration: It includes 4 items that measure productive activities.
The total score of 15 questions ranges from 0 to 29, where the maximum score corresponds to the highest level of integration, and the minimum score corresponds to the lowest level of integration. The score of each question is from 0 to 2. Score 2 indicates maximum integrity in the relevant question, which is how most questions are scored, except for the last 3 questions, which are scored together and range from 0 to 5 [17].
According to Table 2, all the correlations between the LOTCA and CANTAB tests with the community integration were positive, so with the increase in the score of one measure, another measure also increases. The measure of home integration had the most significant linear relationship with the measures of LOTCA’s mental operation and visual perception, respectively. Also, a significant correlation was seen with all three measures of the CANTAB test.
Social integration had a significant positive relationship with all LOTCA measures except visual organization and all CANTAB measures except SOC. Purposeful activities integration also had a significant linear relationship with orientation, visual perception, and motion proxy from LOTCA’s test and only with DMS from CANTAB’s test. In general, there is a correlation between these two tests of community integration, and this test can be used, but this connection is moderate and not strong.
Table 3 presents the intensity and direction of the relationship between CANTAB and LOTCA measures and its prediction by the community integration test measures with the help of linear regression.
According to Table 3, the measure of home integration has a positive significant relationship with all measures of LOTCA and CANTAB. Still, this relationship is significant only with measures of the visual organization of LOTCA and DMS. For example, for one unit increase in the home integration score, on average, the DMS score increases by 1.320 units. In other words, the coefficient of home integration can be equivalent to the measure of the visual organization from LOTCA’s test and DMS from CANTAB’s test.
Table 4 presents the results of examining the intensity and direction of the correlation of the social integration measure with all LOTCA and CANTAB measures. All these relationships were positive, and all measures except SOC had significant relationships.
Based on the investigation of the intensity and the direction of the correlation of the measures, Table 5 presents the purposeful activities integration with all measures of LOTCA and CANTAB. This measure had a significant relationship with orientation, visual perception, and motion proxy from LOTCA’s test and DMS from CANTAB’s test.
Discussion
Regarding the impact of MS on participation, Aronson stated that MS greatly impacts people’s function and quality of daily life. He stated that one of the destructive consequences of this disorder is job loss of 24% to 80% of these patients [8].
Also, Taylor et al. compared the functional and computer tests in a review of the articles of the last 15 years. At first, they reviewed the primary research on this topic. Based on these research studies, they stated that the initial research on comparing computer and functional tests mainly tended towards functional tests due to better performance, accuracy, and participation. In the end, they stated that due to the dispersion of research, it is very difficult to express the correlation between these two tests and suggested more practical investigations [18].
Lashpin, in defense of computer tests, dealt with evaluating the cognitive functions of MS patients. He stated that because traditional methods, such as using functional tests to evaluate patients, are time-consuming and difficult to obtain, it is better to use computer versions of the tests [19]. In another study, Scherer researched several functional tests to measure cognitive functions in patients with MS. He stated that since time and cost savings are always important, the best cognitive test should be chosen for each of the problems of MS patients [20].
Willer B et al. used the community integration questionnaire to investigate the participation status of people with traumatic brain injury after rehabilitation in New York City. The study shows that this test is a good indicator of the participation of people who have received rehabilitation services rather than those who have not received them [21].
Based on our research, which was designed to measure the relationship between two types of computer and functional tests with the participation rate in people with MS, these patients were selected according to the required criteria. For this purpose, the valid and standard computer test CANTAB was used as a computer tool, and the valid and standard LOTCA test was used as a functional tool to investigate the cognitive function in people with MS. Also, the community integration questionnaire was used to check the level of participation of people with MS in daily life.
People were given information about how to complete the tests and the questionnaire. Subsequently, people were randomly classified into odd and even groups to avoid tiredness, and the tests and the questionnaire completion were done two times. After performing the tests, the data were collected and analyzed.
The results indicate a relative and appropriate relationship between the participation questionnaire and both types of computer tests of CANTAB and functional tests of LOTCA. According to the results, the community integration questionnaire showed a greater relationship with the CANTAB computer test than with the LOTCA functional test. By realizing this result, therapists can use computer tests instead of functional tests.
The results of the reviews
Home integration shows the greatest convergence with the SOC test in CANTAB. The SOC test is related to spatial planning, which forces people to use problem-solving strategies and match and visual perception of two sets of stimuli. Also, this test evaluates working memory and shows the frontal lobe’s function [14]. So, according to the results, the SOC test measures the factors considered in home integration better. After SOC, it has the highest convergence with mental operations from the LOTCA test, DMS, and SST from the CANTAB test.
Social integration has the highest convergence with DMS from the CANTAB test. The DMS test evaluates the ability to adapt vision and short-term memory and is sensitive to medial and frontal temporal lobe inputs [14]. Therefore, according to the results, the DMS test is more suitable for evaluating the desired factors in social integration. After DMS, it has the highest convergence with visual perception, motion proxy, and orientation from the LOTCA test.
Purposeful activities integration has the greatest convergence with motion proxy from the LOTCA test. Motion proxy assesses a person’s ability to imitate movement actions, use objects, and perform symbolic actions. Therefore, according to the results, the motion proxy item is better for evaluating the factors considered in purposeful activities integration. Also, purposeful activities integration after motion proxy has the highest convergence with DMS from the CANTAB test and orientation and visual perception from the LOTCA test.
The results obtained from this research can be used to advance previous studies. According to the results of this research, which show a high convergence between two computer and functional tests with the participation rate, the use of both tests can be preferred in certain circumstances.
As mentioned, computer tests provide more accurate results [20], and they are cheaper, but they may be stressful and cause more fatigue for the person [23]. As the rate of participation in computer and functional tests is discussed, some researchers stated that the rate of participation is higher in computer tests [22, 24]. Some say that the physical nature of the screen requires more cognitive processes [25] and fewer keyboard skills [26], and the participation of people in functional tests is more than in computer tests.
A very important point in this regard is the way of grading computer and functional tests. Human agents perform functional tests. Many conditions, such as the way people are graded, can affect the score obtained by a person, while in computer tests, human factors are not involved in scoring, and the person gets an accurate score [27].
Conclusion
According to the results of this research, which show a good convergence between two computer and functional tests with the participation rate, it can be said that the use of both tests can be preferred in certain circumstances.
Ethical Considerations
Compliance with ethical guidelines
In the implementation of the research, ethical considerations were considered following the instructions of the Ethics Committee of University of Social Welfare and Rehabilitation Sciences. These principles included obtaining the written consent of the participants, keeping the information confidential, making the participants aware of the research process, not exposing the participants to risk, and promoting human health while maintaining dignity (Code: IR.USWR.REC.2020.215).
Funding
This study was extracted from the first author’s master’s thesis, Department of Occupational Therapy, University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Conceptualization: Hojat Allah Haqgoo, Ebrahim Peshyareh, Milad Faraji, and Elyas Monfared; Methodology, validation, and sources: Mohsen Vahedi and Milad Faraji; Analysis: Hojat Allah Haqgou, Mohsen Vahedi, and Milad Faraji; Research, review and visualization: Milad Faraji and Elyas Monfared; Financing and writing the draft: Milad Faraji; Research management, editing and finalization: Hojat Allah Haqgoo and Milad Faraji; Supervision: Hojat Allah Haqgoo and Ebrahim Peshyareh.
Conflict of interest
The authors declared no conflict of interest.
References
- Schoonheim MM, Meijer KA, Geurts JJ. Network collapse and cognitive impairment in multiple sclerosis. Frontiers in Neurology. 2015; 6:82. [DOI:10.3389/fneur.2015.00082] [PMID] [PMCID]
- Price CC, Garvan CW, Monk TG. Type and severity of cognitive decline in older adults after noncardiac surgery. Anesthesiology. 2008; 108(1):8-17. [DOI:10.1097/01.anes.0000296072.02527.18] [PMID] [PMCID]
- Correa DD, Maron L, Harder H, Klein M, Armstrong CL, Calabrese P, et al. Cognitive functions in primary central nervous system lymphoma: literature review and assessment guidelines. Annals of Oncology. 2007; 18(7):1145-51. [DOI:10.1093/annonc/mdl464] [PMID]
- Khan F, Amatya B. Rehabilitation in multiple sclerosis: A systematic review of systematic reviews. Archives of physical medicine and rehabilitation. 2017; 98(2):353-67. [DOI:10.1016/j.apmr.2016.04.016] [PMID]
- Law M. Participation in the occupations of everyday life. American Journal of Occupational Therapy. 2002; 56(6):640-9. [DOI:10.5014/ajot.56.6.640] [PMID]
- Chen H-F, Cohn ES. Social participation for children with developmental coordination disorder: Conceptual, evaluation and intervention considerations. Physical & Occupational Therapy in Pediatrics. 2003; 23(4):61-78. [DOI:10.1300/J006v23n04_05]
- Perenboom RJ, Chorus AM. Measuring participation according to the international classification of functioning, disability and health (ICF). Disability and Rehabilitation. 2003; 25(11-12):577-87. [DOI:10.1080/0963828031000137081] [PMID]
- Kielhofner G. Functional Assessment: Toward a dialectical view of person-environment relations. American Journal of Occupational Therapy. 1993; 47(3):248-51. [DOI:10.5014/ajot.47.3.248] [PMID]
- Aronson KJ. Quality of life among persons with multiple sclerosis and their caregivers. Neurology. 1997; 48(1):74-80. [DOI:10.1212/WNL.48.1.74] [PMID]
- Kalmar JH, Gaudino EA, Moore NB, Halper J, DeLuca J. The relationship between cognitive deficits and everyday functional activities in multiple sclerosis. Neuropsychology. 2008; 22(4):442-9. [DOI:10.1037/0894-4105.22.4.442] [PMID]
- Einarsson U, Gottberg K, Fredrikson S, Von Koch L, Holmqvist LW. Activities of daily living and social activities in people with multiple sclerosis in Stockholm county. Clinical Rehabilitation. 2006; 20(6):543-51. [DOI:10.1191/0269215506cr953oa] [PMID]
- Steultjens EM, Dekker J, Bouter LM, Jellema S, Bakker EB, Van Den Ende CH. Occupational therapy for community dwelling elderly people: A systematic review. Age and Ageing. 2004; 33(5):453-60. [DOI:10.1093/ageing/afh174] [PMID]
- Demaree HA, DeLuca J, Gaudino EA, Diamond BJ. Speed of information processing as a key deficit in multiple sclerosis: implications for rehabilitation. Journal of Neurology, Neurosurgery and Psychiatry. 1999; 67(5):661-3. [DOI:10.1136/jnnp.67.5.661] [PMID] [PMCID]
- Hancock LM, Bruce JM, Bruce AS, Lynch SG. Processing speed and working memory training in multiple sclerosis: A double-blind randomized controlled pilot study. Journal of Clinical and Experimental Neuropsychology. 2015; 37(2):113-27. [DOI:10.1080/13803395.2014.989818] [PMID]
- Itzkovich M, Elazar B, Averbuch S. Loewenstein occupational therapy cognitive assessment (LOTCA) manual (2000). Maddak Incorporated. [Link]
- Katz N, Itzkovich M, Averbuch S, Elazar B. Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) battery for brain-injured patients: reliability and validity. American Journal of Occupational Therapy. 1989; 43(3):184-92. [DOI:10.5014/ajot.43.3.184] [PMID]
- Karbalaei-Nouri A, Sadeghi A, Shamsolma’aali Z. Construct validity confirmation of Iranian version of Lowenstein Occupational Therapy Cognitive Assessment (LOTCA) [(Persian)]. Archives of Rehabilitation. 2009; 10(2):0-0. [Link]
- Luciana M, Nelson CA. Assessment of neuropsychological function through use of the cambridge neuropsychological testing automated battery: Performance in 4- to 12-year-old children. Developmental Neuropsychology 2002; 22(3):595-624. [DOI:10.1207/S15326942DN2203_3] [PMID]
- Gualtieri CT, Johnson LG. Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Archives of Clinical Neuropsychology. 2006; 21(7):623-43. [DOI:10.1016/j.acn.2006.05.007] [PMID]
- Torgersen J, Flaatten H, Engelsen BA, Gramstad A. Clinical validation of Cambridge neuropsychological test automated battery in a Norwegian epilepsy population. Journal of Behavioral and Brain Science. 2012; 2(1):108-16. [DOI:10.4236/jbbs.2012.21013]
- Willer B, Ottenbacher KJ, Coad ML. The community integration questionnaire. A comparative examination. American Journal of Physical Medicine & Rehabilitation. 1994; 73(2):103-11. [DOI:10.1097/00002060-199404000-00006] [PMID]
- Negahban H, Fattahizadeh P, Ghasemzadeh R, Salehi R, Majdinasab N, Mazaheri M. The Persian version of community integration questionnaire in persons with multiple sclerosis: translation, reliability, validity, and factor analysis. Disability and Rehabilitation. 2013; 35(17):1453-9. [DOI:10.3109/09638288.2012.741653] [PMID]
- McColl MA, Davies D, Carlson P, Johnston J, Minnes P. The community integration measure: Development and preliminary validation. Archives of Physical Medicine and Rehabilitation. 2001; 82(4):429-34. [DOI:10.1053/apmr.2001.22195] [PMID]
- Noyes JM, Garland KJ. Computer-vs. paper-based tasks: Are they equivalent? Ergonomics. 2008; 51(9):1352-75. [DOI:10.1080/00140130802170387] [PMID]
- Lapshin H, O'Connor P, Lanctôt KL, Feinstein A. Computerized cognitive testing for patients with multiple sclerosis. Multiple Sclerosis and Related Disorders. 2012; 1(4):196-201. [DOI:10.1016/j.msard.2012.05.001] [PMID]
- Scherer P. Cognitive screening in multiple sclerosis. Journal of Neurology. 2007; 254(Suppl 2):II26-9. [DOI:10.1007/s00415-007-2008-3] [PMID]
- Willer B, Rosenthal M, Kreutzer JS, Gordon WA, Rempel R. Assessment of community integration following rehabilitation for traumatic brain injury. The Journal of Head Trauma Rehabilitation. 1993; 8(2):75-87. [DOI:10.1097/00001199-199308020-00009]
- Olsen JB, Maynes DD, Slawson D, Ho K. Comparisons of paper-administered, computer-administered and computerized adaptive achievement tests. Journal of Educational Computing Research. 1989; 5(3):311-26. [DOI:10.2190/86RK-76WN-VAJ0-PFA3]
- Wästlund E, Reinikka H, Norlander T, Archer T. Effects of VDT and paper presentation on consumption and production of information: Psychological and physiological factors. Computers in Human Behavior. 2005; 21(2):377-94. [DOI:10.1016/j.chb.2004.02.007]
- Greaud VA, Green BF. Equivalence of conventional and computer presentation of speed tests. Applied Psychological Measurement. 1986;10(1):23-34. [DOI:10.1177/014662168601000102]
- Ziefle M. Effects of display resolution on visual performance. Human Factors. 1998; 40(4):554-68. [DOI:10.1518/001872098779649355] [PMID]
- Russell M. Testing on computers. Education Policy Analysis Archives. 1999; 7:20. [DOI:10.14507/epaa.v7n20.1999]
- Angelo J, Smith RO. An analysis of computer-related articles in occupational therapy periodicals. American Journal of Occupational Therapy. 1993;47(1):25-9. [DOI:10.5014/ajot.47.1.25] [PMID]
Type of Study: Original |
Subject:
Occupational Therapy
Received: 19/08/2021 | Accepted: 11/12/2021 | Published: 1/01/2023
Received: 19/08/2021 | Accepted: 11/12/2021 | Published: 1/01/2023
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
