

Volume 23, Issue 1 (5-2022)
Arch Rehabil 2022, 23(1): 8-31 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Soleimani F, Azari N, Vameghi R, Barekati S H, Lornejad H, Kraskian A. Standardization of the Bayley Scales of Infant and Toddler Development for Persian Children. Arch Rehabil 2022; 23 (1) :8-31
URL: http://rehabilitationj.uswr.ac.ir/article-1-2890-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-2890-en.html
Farin Soleimani1  , Nadia Azari *2 , Roshanak Vameghi3 , Seyyed Hamed Barekati4 , Hamidreza Lornejad4 , Adis Kraskian5
, Nadia Azari *2 , Roshanak Vameghi3 , Seyyed Hamed Barekati4 , Hamidreza Lornejad4 , Adis Kraskian5
, Nadia Azari *2 , Roshanak Vameghi3 , Seyyed Hamed Barekati4 , Hamidreza Lornejad4 , Adis Kraskian5
1- Pediatric Neurorehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran., Kodakyar Ave., Daneshjo Blvd., Evin, Post code: 1985713871 Telephone and Fax number: 009821-71732846.
2- Pediatric Neurorehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,Farinir@Yahoo.com
3- Department of Clinical Education, Pediatric Neurorehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran., Kodakyar Ave., Daneshjo Blvd., Evin, Post code: 1985713871 Telephone and Fax number: 009821-71732846.
4- Ministry of Health and Medical Education, Tehran, Iran., Iran Ministry of Health and Medical Education, Tehran, Iran.
5- Department of psychology, Islamic Azad University, Branch of Karaj, Karaj, Iran., Department of psychology, Islamic Azad University, Branch of Karaj, Karaj, Iran.
2- Pediatric Neurorehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
3- Department of Clinical Education, Pediatric Neurorehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran., Kodakyar Ave., Daneshjo Blvd., Evin, Post code: 1985713871 Telephone and Fax number: 009821-71732846.
4- Ministry of Health and Medical Education, Tehran, Iran., Iran Ministry of Health and Medical Education, Tehran, Iran.
5- Department of psychology, Islamic Azad University, Branch of Karaj, Karaj, Iran., Department of psychology, Islamic Azad University, Branch of Karaj, Karaj, Iran.
Keywords: Child, Developmental delay, Standardization, Bayley Scales of Infants and Toddlers Development
Full-Text [PDF 2583 kb]
(2433 Downloads)
| Abstract (HTML) (6681 Views)
Full-Text: (5542 Views)
Introduction
The childhood years are the most vital years of life which make the foundation of future life when humans experience developments in Cognition, motor, language, emotional, and social domains [1, 2]. More than 200 million children in developing countries, i.e, more than one-third of children worldwide, do not experience proper development. As a result, their countries lose approximately 20% of their manpower [3]. The critical period for growth and development is during the early years of childhood (first 5 years) [4]. To ensure optimal development, a growth assessment in early childhood is needed; therefore, developmental screening for timely interventions in early childhood can reduce the incidence of developmental delay [5, 6, 7, 8, 9]. About 6-9% of children under 6 years of age suffer from developmental delay or disorders and need early intervention [10, 11, 12, 13, 14]. An study in the United States (US) indicated that 1 in 6 children with developmental disorders have speech and language disorders, mental retardation, cerebral palsy, and autism [11]. Most children who need early intervention are not diagnosed before school age [9, 15]. Children whose developmental delay is undiagnosed and, consequently, receive no intervention until school age are at risk for academic failure, behavioral problems, and socio-emotional disorders [16].
The World Health Organization has emphasizes that the provision of better care in early childhood improves the child’s school performance [17, 18, 19]. To definitively diagnose children with developmental disorders, valid and reliable tools should be used. In developing countries, the tools developed by developed countries are often used. These tools include items that may be adaptable to other cultures. Hence, the tools may fail to assess children from different cultures [20]. These tools should be translated and localized to be adaptable to other cultures [21]. On the other hand, the use of norm scores based on the original version of the tools can lead to errors in estimating the developmental level of children in other countries; therefore, determining the norm scores for different cultures is necessary [22].
The standardization of developmental tests for children is limited in Iran; the ages & stages questionnaire (ASQ) [24] and the Denver Developmental Screening Test [25] have been translated and their validity and reliability have been examined, but their norm scores have not been determined. The bayley scales of infant and toddler development, third edition (Bayley-III) assesses the child’s developmental status in five developmental domains including cognition, language (receptive, expressive communication), motor (gross and fine), social-emotional, and adaptive behavior in early childhood, i.e, from day 15 to 42 months. It is used as the gold standard for grading other developmental assessment tools [23], and is applied in many countries. In a study, it was found reliance on US norm-based scores of Bayley-III led to the misclassification of developmental delays in Malawian children [26]. A study conducted in Taiwan suggested that higher Bayley-III scores should be considered in Taiwanese children as a sign of developmental delay [27]. Godamunne used cognition and motor subscales of Bayley-III for Sri Lankan children and compared their performance with US children based on the subscales. The results showed that the scores of 12-month-old children were higher in the cognition domain and lower in the motor domain compared to the US children, while the scores of 24-month-old children were lower in the cognition domain compared to the US children [28]. In another study which was conducted on preterm infants, it was warned that we should be cautious in interpreting Bayley-III scores for detecting developmental delays in this group and the norm scores of this test should be considered higher than US norm-based scores [29].
Since a comprehensive and appropriate test is not available for health care providers in Iran to assess the development status of children in various fields and be used as a gold standard, and given that the use of scores based on the norms of a country may lead to the wrong estimation of disorders in other countries, this study aims to standardize the Bayley-III for Iranian children. The mean raw scores in the two main and Persian versions were examined to compare the development level of US and Iranian children.
Materials and Methods
Study design and participants
This is a cross-sectional study. Sampling was conducted using a stratified sampling method. First, Iran was divided into eight geographical zones (center, north, west, south, southeast, southwest, northeast, northwest, and center) and 10 cities including Tehran, Isfahan, Mashhad, Rasht, Tabriz, Hamadan, Ahvaz , Shiraz, Qom, and Zahedan were selected. Two experienced childcare experts from each city were selected for training and testing. The sampling phase lasted for 3-6 months, depending on the population rate of different cities. The selected samples were 1700 children aged 16 days to 42 months 15 days including 17 age groups of 100 samples from A to Q. The age range was categorized into 1-6 months groups with a one-month interval, 6-12 months group with a two-months interval, 12-30 months group with a 3-month interval, and 30-42 months group with a 6-month interval. This sample size was calculated based on the 2011 national population and housing census related to the population aged <4 years for each city [30]which are presented in Table 1.
.jpg)
The samples were classified based on demographic factors including age, gender, and geographical area. Inclusion criteria were no significant medical complications and not being under treatment for any cognition, physical, or behavioral problems. Exclusion criteria were attendance in rehabilitation interventions, being unable to speak in Persian, and having sensory disorders. After receiving written consent from the parents of children, they completed a demographic form (surveying child’s age and gender, parents’ education, gestational age at birth, birth weight, birth defects). In case of a developmental delay, the child was introduced to the Integrated Center for Child Development for diagnostic measures and health promotion training.
Data collection
The Bayley-III is an assessment tool that evaluates developmental level of children in 5 domains including cognition (91 items), receptive communication (49 items), expressive communication (48 items), fine motor (66 items), and gross motor (72 items). Norm data of this test were achieved from 1700 samples in the US version [23]. The assessment was conducted objectively by the examiner. The norm scores were determined for 48 age groups to increase the accuracy. The test reports four groups of norm scores: Scaled scores, composite scores, percentile ranks, and growth scores. Confidence intervals are provided for these scores, and developmental age equivalents are available for the relevant scales. The Persian version of Bayley-III was used in this study. The Cronbach’s alpha coefficients for all domains are higher than 0.76 and the Pearson correlation coefficient in the test-retest method and inter-rater method for different domains was 0.987 (P<0.001) and 0.991 (P<0.001), respectively [31].
Data analysis
At first, 48 age groups were determined based on the available samples. To determine norm scores from the main version; i.e, the conversion of raw scores into scaled, composite, and growth scores, the percentile ranks and developmental age equivalents were used at 48 age groups from 15 days to 42 months. The scaled scores obtained from the raw scores were converted linearly into scores in the range of 1-19 with a Mean±SD of 10±3. The composite scores were derived from the sums scores of the subscales and converted into a score of 40-160 with a Mean±SD of 100±15. The percentile scores were converted into a score of 1-99 with a mean of 50. The sums percentile ranks (range from 1 to 99, with 50 as the mean and median), and 90% and 95% confidence intervals were determined for cognition, language, and motor subscales. The growth scores were obtained by converting raw scores to scores in the range of 200-800 with a mean of 500 and a SD of 100. Accordingly, the growth curves were plotted to show the child’s growth over time for cognition, receptive and expressive communications and fine and gross motors at 5, 10, 25, 50, 75, 90, and 95 percentiles. To determine the developmental age equivalent, the raw score which was equivalent to the score of 10 for each age group, was calculated. To compare the developmental level of the US and Iranian children, their mean raw scores were examined in five domains at 48 age groups, and the difference in scores was statistically evaluated.
Results
In this study, participants were 1744 children aged 15 days to 42 months; 908 girls (52.1%) and 836 boys (47.9%). Their norm scores based on the Bayley-III were determined in 48 age groups. Based on the parents’ educational level, 64.5%, 34.2%, and 1.3% of fathers, and 58%, 41%, and 1% of mothers had diploma and lower, bachelor’s degree, master’s degree and higher, respectively. Table 2 presents the mean raw scores and SD for the Bayley-III subscales in the norm sample for 17 age groups.
.jpg)
The norm scores in 48 age groups based on composite score, percentile rank, and developmental age equivalent for cognition, receptive and expressive communications, gross motor, and fine motor were also obtained. Results in Table 3 showed a significant difference between the US and Iranian children.

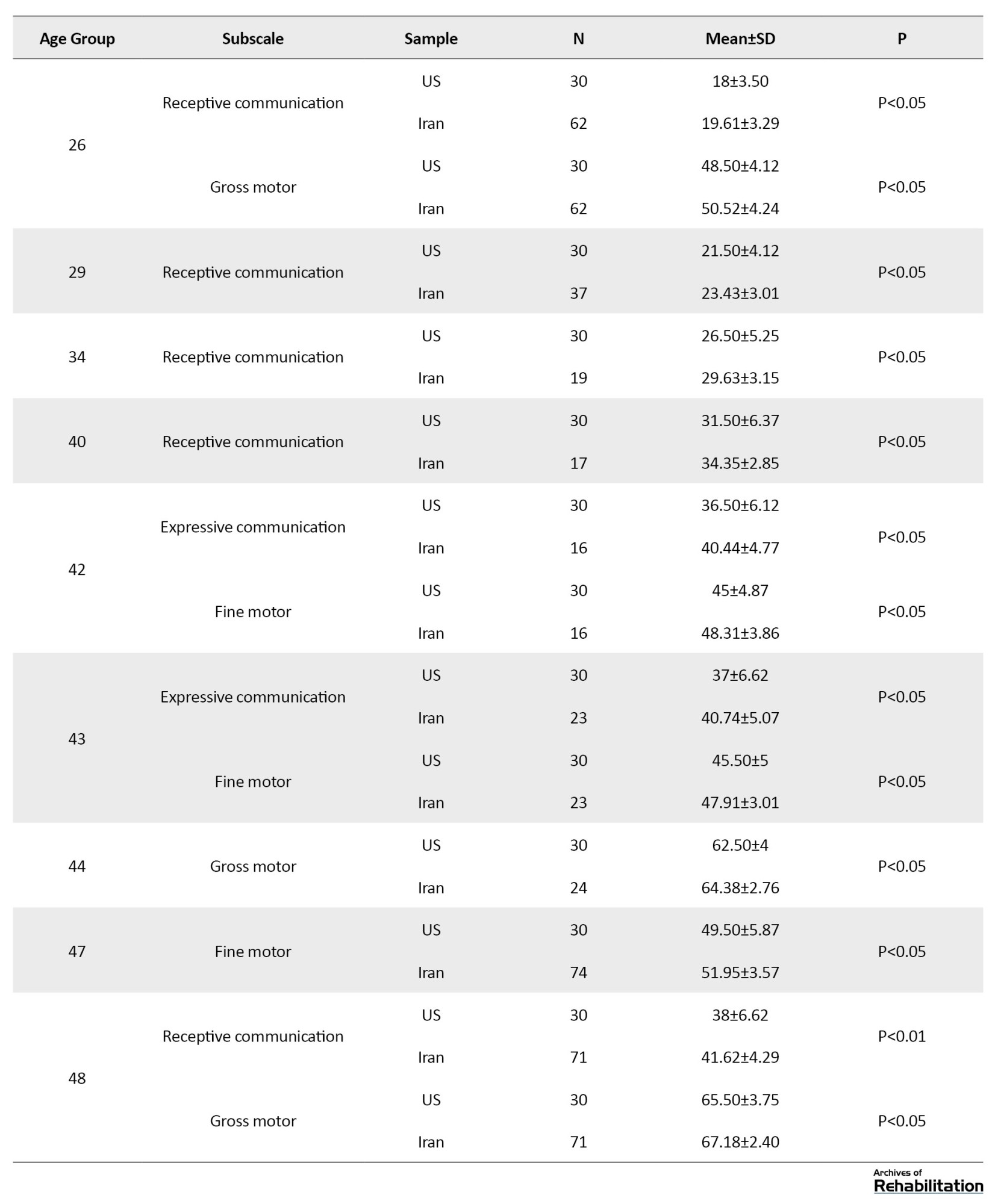
The mean scores at 28 age groups (2 in cognition, 12 in receptive communication, 3 in receptive communication, 4 in fine motor, and 7 in gross motor) were different between the two groups.
Discussion and Conclusion
In this study, the Bayley-III score was normalized in a sample of 1744 children aged 1-42 months in Iran. Norm scores (scaled, composite, and growth scores) were calculated, and the percentile ranks and developmental age equivalent of Iranian children were determined. The difference in mean norm scores in 28 age groups was different between the US and Iranian samples (P<0.05). In 7 age groups, the mean norm scores were higher than in the US children (age range <6 months) while in 21 age groups, the mean norm scores were higher than in the Iranian children (age range >6 months). In this study, only children with normal development were included. Since the US samples are representative of the general population, about 10% of the samples were devoted to children with special needs (21 children with trisomy, cerebral palsy, autism spectrum disorder, prematurity, specific speech disorders, maternal alcohol consumption during pregnancy, asphyxia at birth, and low birth weight) [23]. Previous studies have indicated that the inclusion of children with special needs in a standard sample can negatively affect the ability to distinguish children with natural development and developmental delay [32]. For this reason, this technqiue was not used in our study. The selection of normal children in Iran may have caused an increase in the mean scores, a difference between the US and Iranian samples, or a difference in biological, environmental, and cultural characteristics. The same differences between the two norms have been identified in the studies conducted in other countries [26, 27, 28 ,29, 33, 34].
In Iran, only the ASQ score has been normalized [24]. The ASQ has communication, fine motor, gross motor, problem-solving and personal-social domains for the ages of 4-60 months, which is completed by parents. Examining the difference between the mean scores of the Iranian and US children reported that the scores of Iranian children in the areas of fine motor, problem-solving and personal-social, especially at the ages of 8 and 12 months, were higher than those of the US children, while in the gross motor domain, especially at 36 months, their scores were lower than the US children (P<0.05) [24]. In our study, the mean scores of all Bayley-III subscales for the age group >6 months were higher in the Iranian children compared to the US children. In the Netherlands, the Bayley-III norm scores were obtained at 48 age groups for cognition, motor, and language scales. The mean scores of Dutch and US children were different. It was reported that the use of US norm-based scores in the Netherlands leads to the lack of early detection of developmental delay in children [35].
Cromwell et al. examined the validity of Bayley-III in Mali. They performed the test on 167 healthy Malawian children. The results indicated that the mean scores of Malawian children under the age of 6 months were higher than those of US peers in all subscales; however, the US children showed higher scores at the ages above 6 months [26]. Moore evaluated 185 children aged 29-41 months simultaneously with the Bayley-II and Bayley-III tools. Their results indicated that the development level of children’s cognition and communication based on the Bayley-III score was higher than that based on the Bayley-II score. They suggested that it should be careful in using the Bayley-III scores to detect developmental delays in children [29].
Similarly, Johnson et al. conducted a study on 158 preterm childs to assess how to classify neurodevelopmental delay using Bayley-III compared to the Bayley-II. The scores obtained by the Bayley-III were higher than those by the Bayley-II [33]. In Taiwan, Yu et al. used the Bayley-II and Bayley-III simultaneously in 47 norm infants and 167 preterm infants at the ages of 6, 12, 18, and 24 months. They stated that the scores obtained from the Bayley-III determined the development level of Taiwanese children higher compared to the scores of Bayley-II [27]. Anderson et al. evaluated the Bayley-III’s ability to diagnose developmental delay in 2-year-old children born prematurely (aged <28 weeks) or underweight (weight <1,000 grams) in Victoria, Australia. The mean of all subscale scores in the patient group was significantly lower than in the control group. However, their mean scores were consistent with the mean scores of the US samples; the mean scores in the control group were higher than in the US samples. They concluded that the US children’s Bayley III scores underestimated the developmental delay in Australia [34]. Godamunne et al. used the cognition and motor domains of the Bayley-III in 150 Sri Lankan norm children in 6-, 12-, and 24-month-old age groups and compared their performance with the US children. The results showed that the cognition score of 12-month-old children was higher and their motor scores were lower compared to the US children, and the cognition score of 24-month-old children was lower than that of the US children [28].
The Bayley-III is apropriate for assessment of child development, because of its good psychometric properties and quantitative scoring system. The standardization of its Persian version not only allows early detection of developmental delay, but also eliminates the lack of a gold standard for comparing the results of other developmental tests in Iran.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences. Informed consent was obtained from the parents of the children (Code: IR.USWR.REC.1393.14357).
Funding
Financial support for this study was obtained from the Iranian Ministry of Health and Medical Education.
Authors' contributions
Conceptualization: Farin Soleimani, Nadia Azari, RoshanakVameghi;Methodology: Farin Soleimani, NadiaAzari, Adis Kraskian; Investigation: Farin Soleimani,Nadia Azari, Seyed Hamed barekati, Hamidreza Lornejad;Writing-original draft: Farin Soleimani, Nadia Azari;Writing-review & editing: All author.
Conflict of interest
According to the authors, there is no conflict of interest.
Acknowledgments
The authors would like to thank the University of Social Welfare and Rehabilitation Sciences and the Shahid Beheshti University of Medical Sciences, Iran, Tehran, Mashhad, Rasht, Tabriz, Hamedan, Ahvaz, Shiraz, Isfahan, Qom, and Zahedan for their cooperation and the parents of children who participated in the study.
References
The childhood years are the most vital years of life which make the foundation of future life when humans experience developments in Cognition, motor, language, emotional, and social domains [1, 2]. More than 200 million children in developing countries, i.e, more than one-third of children worldwide, do not experience proper development. As a result, their countries lose approximately 20% of their manpower [3]. The critical period for growth and development is during the early years of childhood (first 5 years) [4]. To ensure optimal development, a growth assessment in early childhood is needed; therefore, developmental screening for timely interventions in early childhood can reduce the incidence of developmental delay [5, 6, 7, 8, 9]. About 6-9% of children under 6 years of age suffer from developmental delay or disorders and need early intervention [10, 11, 12, 13, 14]. An study in the United States (US) indicated that 1 in 6 children with developmental disorders have speech and language disorders, mental retardation, cerebral palsy, and autism [11]. Most children who need early intervention are not diagnosed before school age [9, 15]. Children whose developmental delay is undiagnosed and, consequently, receive no intervention until school age are at risk for academic failure, behavioral problems, and socio-emotional disorders [16].
The World Health Organization has emphasizes that the provision of better care in early childhood improves the child’s school performance [17, 18, 19]. To definitively diagnose children with developmental disorders, valid and reliable tools should be used. In developing countries, the tools developed by developed countries are often used. These tools include items that may be adaptable to other cultures. Hence, the tools may fail to assess children from different cultures [20]. These tools should be translated and localized to be adaptable to other cultures [21]. On the other hand, the use of norm scores based on the original version of the tools can lead to errors in estimating the developmental level of children in other countries; therefore, determining the norm scores for different cultures is necessary [22].
The standardization of developmental tests for children is limited in Iran; the ages & stages questionnaire (ASQ) [24] and the Denver Developmental Screening Test [25] have been translated and their validity and reliability have been examined, but their norm scores have not been determined. The bayley scales of infant and toddler development, third edition (Bayley-III) assesses the child’s developmental status in five developmental domains including cognition, language (receptive, expressive communication), motor (gross and fine), social-emotional, and adaptive behavior in early childhood, i.e, from day 15 to 42 months. It is used as the gold standard for grading other developmental assessment tools [23], and is applied in many countries. In a study, it was found reliance on US norm-based scores of Bayley-III led to the misclassification of developmental delays in Malawian children [26]. A study conducted in Taiwan suggested that higher Bayley-III scores should be considered in Taiwanese children as a sign of developmental delay [27]. Godamunne used cognition and motor subscales of Bayley-III for Sri Lankan children and compared their performance with US children based on the subscales. The results showed that the scores of 12-month-old children were higher in the cognition domain and lower in the motor domain compared to the US children, while the scores of 24-month-old children were lower in the cognition domain compared to the US children [28]. In another study which was conducted on preterm infants, it was warned that we should be cautious in interpreting Bayley-III scores for detecting developmental delays in this group and the norm scores of this test should be considered higher than US norm-based scores [29].
Since a comprehensive and appropriate test is not available for health care providers in Iran to assess the development status of children in various fields and be used as a gold standard, and given that the use of scores based on the norms of a country may lead to the wrong estimation of disorders in other countries, this study aims to standardize the Bayley-III for Iranian children. The mean raw scores in the two main and Persian versions were examined to compare the development level of US and Iranian children.
Materials and Methods
Study design and participants
This is a cross-sectional study. Sampling was conducted using a stratified sampling method. First, Iran was divided into eight geographical zones (center, north, west, south, southeast, southwest, northeast, northwest, and center) and 10 cities including Tehran, Isfahan, Mashhad, Rasht, Tabriz, Hamadan, Ahvaz , Shiraz, Qom, and Zahedan were selected. Two experienced childcare experts from each city were selected for training and testing. The sampling phase lasted for 3-6 months, depending on the population rate of different cities. The selected samples were 1700 children aged 16 days to 42 months 15 days including 17 age groups of 100 samples from A to Q. The age range was categorized into 1-6 months groups with a one-month interval, 6-12 months group with a two-months interval, 12-30 months group with a 3-month interval, and 30-42 months group with a 6-month interval. This sample size was calculated based on the 2011 national population and housing census related to the population aged <4 years for each city [30]which are presented in Table 1.
The samples were classified based on demographic factors including age, gender, and geographical area. Inclusion criteria were no significant medical complications and not being under treatment for any cognition, physical, or behavioral problems. Exclusion criteria were attendance in rehabilitation interventions, being unable to speak in Persian, and having sensory disorders. After receiving written consent from the parents of children, they completed a demographic form (surveying child’s age and gender, parents’ education, gestational age at birth, birth weight, birth defects). In case of a developmental delay, the child was introduced to the Integrated Center for Child Development for diagnostic measures and health promotion training.
Data collection
The Bayley-III is an assessment tool that evaluates developmental level of children in 5 domains including cognition (91 items), receptive communication (49 items), expressive communication (48 items), fine motor (66 items), and gross motor (72 items). Norm data of this test were achieved from 1700 samples in the US version [23]. The assessment was conducted objectively by the examiner. The norm scores were determined for 48 age groups to increase the accuracy. The test reports four groups of norm scores: Scaled scores, composite scores, percentile ranks, and growth scores. Confidence intervals are provided for these scores, and developmental age equivalents are available for the relevant scales. The Persian version of Bayley-III was used in this study. The Cronbach’s alpha coefficients for all domains are higher than 0.76 and the Pearson correlation coefficient in the test-retest method and inter-rater method for different domains was 0.987 (P<0.001) and 0.991 (P<0.001), respectively [31].
Data analysis
At first, 48 age groups were determined based on the available samples. To determine norm scores from the main version; i.e, the conversion of raw scores into scaled, composite, and growth scores, the percentile ranks and developmental age equivalents were used at 48 age groups from 15 days to 42 months. The scaled scores obtained from the raw scores were converted linearly into scores in the range of 1-19 with a Mean±SD of 10±3. The composite scores were derived from the sums scores of the subscales and converted into a score of 40-160 with a Mean±SD of 100±15. The percentile scores were converted into a score of 1-99 with a mean of 50. The sums percentile ranks (range from 1 to 99, with 50 as the mean and median), and 90% and 95% confidence intervals were determined for cognition, language, and motor subscales. The growth scores were obtained by converting raw scores to scores in the range of 200-800 with a mean of 500 and a SD of 100. Accordingly, the growth curves were plotted to show the child’s growth over time for cognition, receptive and expressive communications and fine and gross motors at 5, 10, 25, 50, 75, 90, and 95 percentiles. To determine the developmental age equivalent, the raw score which was equivalent to the score of 10 for each age group, was calculated. To compare the developmental level of the US and Iranian children, their mean raw scores were examined in five domains at 48 age groups, and the difference in scores was statistically evaluated.
Results
In this study, participants were 1744 children aged 15 days to 42 months; 908 girls (52.1%) and 836 boys (47.9%). Their norm scores based on the Bayley-III were determined in 48 age groups. Based on the parents’ educational level, 64.5%, 34.2%, and 1.3% of fathers, and 58%, 41%, and 1% of mothers had diploma and lower, bachelor’s degree, master’s degree and higher, respectively. Table 2 presents the mean raw scores and SD for the Bayley-III subscales in the norm sample for 17 age groups.
The norm scores in 48 age groups based on composite score, percentile rank, and developmental age equivalent for cognition, receptive and expressive communications, gross motor, and fine motor were also obtained. Results in Table 3 showed a significant difference between the US and Iranian children.
The mean scores at 28 age groups (2 in cognition, 12 in receptive communication, 3 in receptive communication, 4 in fine motor, and 7 in gross motor) were different between the two groups.
Discussion and Conclusion
In this study, the Bayley-III score was normalized in a sample of 1744 children aged 1-42 months in Iran. Norm scores (scaled, composite, and growth scores) were calculated, and the percentile ranks and developmental age equivalent of Iranian children were determined. The difference in mean norm scores in 28 age groups was different between the US and Iranian samples (P<0.05). In 7 age groups, the mean norm scores were higher than in the US children (age range <6 months) while in 21 age groups, the mean norm scores were higher than in the Iranian children (age range >6 months). In this study, only children with normal development were included. Since the US samples are representative of the general population, about 10% of the samples were devoted to children with special needs (21 children with trisomy, cerebral palsy, autism spectrum disorder, prematurity, specific speech disorders, maternal alcohol consumption during pregnancy, asphyxia at birth, and low birth weight) [23]. Previous studies have indicated that the inclusion of children with special needs in a standard sample can negatively affect the ability to distinguish children with natural development and developmental delay [32]. For this reason, this technqiue was not used in our study. The selection of normal children in Iran may have caused an increase in the mean scores, a difference between the US and Iranian samples, or a difference in biological, environmental, and cultural characteristics. The same differences between the two norms have been identified in the studies conducted in other countries [26, 27, 28 ,29, 33, 34].
In Iran, only the ASQ score has been normalized [24]. The ASQ has communication, fine motor, gross motor, problem-solving and personal-social domains for the ages of 4-60 months, which is completed by parents. Examining the difference between the mean scores of the Iranian and US children reported that the scores of Iranian children in the areas of fine motor, problem-solving and personal-social, especially at the ages of 8 and 12 months, were higher than those of the US children, while in the gross motor domain, especially at 36 months, their scores were lower than the US children (P<0.05) [24]. In our study, the mean scores of all Bayley-III subscales for the age group >6 months were higher in the Iranian children compared to the US children. In the Netherlands, the Bayley-III norm scores were obtained at 48 age groups for cognition, motor, and language scales. The mean scores of Dutch and US children were different. It was reported that the use of US norm-based scores in the Netherlands leads to the lack of early detection of developmental delay in children [35].
Cromwell et al. examined the validity of Bayley-III in Mali. They performed the test on 167 healthy Malawian children. The results indicated that the mean scores of Malawian children under the age of 6 months were higher than those of US peers in all subscales; however, the US children showed higher scores at the ages above 6 months [26]. Moore evaluated 185 children aged 29-41 months simultaneously with the Bayley-II and Bayley-III tools. Their results indicated that the development level of children’s cognition and communication based on the Bayley-III score was higher than that based on the Bayley-II score. They suggested that it should be careful in using the Bayley-III scores to detect developmental delays in children [29].
Similarly, Johnson et al. conducted a study on 158 preterm childs to assess how to classify neurodevelopmental delay using Bayley-III compared to the Bayley-II. The scores obtained by the Bayley-III were higher than those by the Bayley-II [33]. In Taiwan, Yu et al. used the Bayley-II and Bayley-III simultaneously in 47 norm infants and 167 preterm infants at the ages of 6, 12, 18, and 24 months. They stated that the scores obtained from the Bayley-III determined the development level of Taiwanese children higher compared to the scores of Bayley-II [27]. Anderson et al. evaluated the Bayley-III’s ability to diagnose developmental delay in 2-year-old children born prematurely (aged <28 weeks) or underweight (weight <1,000 grams) in Victoria, Australia. The mean of all subscale scores in the patient group was significantly lower than in the control group. However, their mean scores were consistent with the mean scores of the US samples; the mean scores in the control group were higher than in the US samples. They concluded that the US children’s Bayley III scores underestimated the developmental delay in Australia [34]. Godamunne et al. used the cognition and motor domains of the Bayley-III in 150 Sri Lankan norm children in 6-, 12-, and 24-month-old age groups and compared their performance with the US children. The results showed that the cognition score of 12-month-old children was higher and their motor scores were lower compared to the US children, and the cognition score of 24-month-old children was lower than that of the US children [28].
The Bayley-III is apropriate for assessment of child development, because of its good psychometric properties and quantitative scoring system. The standardization of its Persian version not only allows early detection of developmental delay, but also eliminates the lack of a gold standard for comparing the results of other developmental tests in Iran.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences. Informed consent was obtained from the parents of the children (Code: IR.USWR.REC.1393.14357).
Funding
Financial support for this study was obtained from the Iranian Ministry of Health and Medical Education.
Authors' contributions
Conceptualization: Farin Soleimani, Nadia Azari, RoshanakVameghi;Methodology: Farin Soleimani, NadiaAzari, Adis Kraskian; Investigation: Farin Soleimani,Nadia Azari, Seyed Hamed barekati, Hamidreza Lornejad;Writing-original draft: Farin Soleimani, Nadia Azari;Writing-review & editing: All author.
Conflict of interest
According to the authors, there is no conflict of interest.
Acknowledgments
The authors would like to thank the University of Social Welfare and Rehabilitation Sciences and the Shahid Beheshti University of Medical Sciences, Iran, Tehran, Mashhad, Rasht, Tabriz, Hamedan, Ahvaz, Shiraz, Isfahan, Qom, and Zahedan for their cooperation and the parents of children who participated in the study.
References
- National Research Council (US) and Institute of Medicine (US) Committee on Integrating the Science of Early Childhood Development. From Neurons to Neighborhoods: The science of early childhood development. Shonkoff JP, Phillips DA, editors. Washington (DC): National Academies Press (US); 2000. [PMID]
- Black J, Jones T, Nelson C, Greenough W. Neuronal plasticity and the developing brain. Handbook of child and adolescent psychiatry, vol 1. New York: Wiley, 1998. pp: 31-53. [Link]
- Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B, et al. Developmental potential in the first 5 years for children in developing countries. The Lancet. 2007; 369(9555):60-70. [DOI:10.1016/S0140-6736(07)60032-4]
- Williams J, Holmes CA. Improving the early detection of children with subtle developmental problems. Journal of Child Health Care. 2004; 8(1):34-46. [DOI:10.1177/1367493504041852] [PMID]
- Glascoe FP. Early detection of developmental and behavioral problems. Pediatrics in Review. 2000; 21(8):272-9; quiz 280. [DOI:10.1542/pir.21.8.272] [PMID]
- Blauw-Hospers CH, Hadders-Algra, M. A systematic review of the effects of early intervention on motor development. Developmental Medicine and Child Neurology. 2005; 47(6):421-32. [PMID]
- Cameron EC, Maehle V, Reid J. The effects of an early physical therapy intervention for very preterm, very low birth weight infants: A randomized controlled clinical trial. Pediatric Physical Therapy. 2005; 17(2):107-19. [DOI:10.1097/01.PEP.0000163073.50852.58] [PMID]
- Guralnick MJ. Early intervention for children with intellectual disabilities: Current knowledge and future prospects. Journal of Applied Research in Intellectual Disabilities. 2005; 18(4):313-24. [DOI:10.1111/j.1468-3148.2005.00270.x]
- Malekpour M. Low birth-weight infants and the importance of early intervention: enhancing mother-infant interactions a literature review. The British Journal of Development Disabilities. 2004; 50(99):78-88. [DOI:10.1179/096979504799103868.]
- Boyle CA, Decoufle P, Yeargin-Allsopp M. Prevalence and health impact of developmental disabilities in US children. Pediatrics. 1994; 93(3):399-403. [DOI:10.1542/peds.93.3.399] [PMID]
- Bloom B, Jones LI, Freeman G. Summary health statistics for U.S. children: National Health Interview Survey, 2002. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. 2002; 10(258):1-81. [Link]
- Wing L, Potter D. The epidemiology of autistic spectrum disorders: Is the prevalence rising? Mental Retardation and Developmental Disabilities Research Reviews. 2002; 8(3):151-61. [DOI:10.1002/mrdd.10029] [PMID]
- National Center for Education Statistics. The Condition of Education. United States, U.S. Department of Education, Office of Educational Research and Improvement, National Center for Education Statistics, 2007. [Link]
- Council on Children With Disabilities; Section on Developmental Behavioral Pediatrics; Bright Futures Steering Committee; Medical Home Initiatives for Children With Special Needs Project Advisory Committee. Identifying infants and young children with developmental disorders in the medical home: An algorithm for developmental surveillance and screening. Pediatrics 2006; 118(1):405-20. [DOI:10.1542/peds.2006-1231] [PMID]
- Palfrey JS, Singer JD, Walker DK, Butler JA. Early identification of children’s special needs: A study in five metropolitan communities. The Journal of Pediatrics. 1987; 111(5):651-9. [DOI:10.1016/S0022-3476(87)80238-X]
- Barnett WS. Long-term effects of early childhood programs on cognitive and school outcomes. The Future of Children. 1995; 5(3):25-50. [DOI:10.2307/1602366]
- World Health Organization (WHO). Department of Maternal, Newborn, Child and Adolescent Health (MCA). [Link]
- No Authors. Developmental surveillance and screening of infants and young children. Pediatrics. 2001; 108(1):192-6. [DOI:10.1542/peds.108.1.192] [PMID]
- Shonkoff JP, Meisels SJ. Handbook of early childhood intervention. Cambridge: Cambridge University Press; 2000. [Link]
- Olade RA. Evaluation of the Denver developmental screening test as applied to African children. Nursing Research. 1984; 33(4):204-7. [DOI:10.1097/00006199-198407000-00005]
- Geisinger KF. Cross-cultural normative assessment: Translation and adaptation issues influencing the normative interpretation of assessment instruments. Psychological Assessment. 1994; 6(4):304-12. [DOI:10.1037/1040-3590.6.4.304]
- Lim HC, Chan T, Yoong T. Standardisation and adaptation of the Denver Developmental Screening Test (DDST) and Denver II for use in Singapore children. Singapore Medical Journal. 1994; 35(2):156-60. [PMID]
- Bayley N. Bayley scales of infant development and toddler development. London: Pearson; 2006. [DOI:10.1037/t14978-000]
- Vameghi R, Sajedi F, Kraskian Mojembari A, Habiollahi A, Lornezhad HR, Delavar B. Cross-Cultural Adaptation, Validation and Standardization of Ages and Stages Questionnaire (ASQ) in Iranian children. Iranian Journal of Public Health. 2013; 42(5):522-8. [PMID]
- Shahshahani S, Vameghi R, Azari N, Sajedi F, Kazemnejad A. Validity and Reliability Determination of Denver Developmental Screening Test-II in 0-6 Year-Olds in Tehran. Iranian Journal of Pediatrics. 2010; 20(3):313-22. [PMID]
- Cromwell EA, Dube Q, Cole SR, Chirambo C, Dow AE, Heyderman RS, et al. Validity of US norms for the Bayley Scales of Infant Development-III in Malawian children. European Journal of Paediatric Neurology. 2014; 18(2):223-30. [DOI:10.1016/j.ejpn.2013.11.011] [PMID] [PMCID]
- Yu YT, Hsieh WS, Hsu CH, Chen LC, Lee WT, Chiu NC, et al. A psychometric study of the Bayley Scales of Infant and Toddler Development - 3rd Edition for term and preterm Taiwanese infants.Research in Developmental Disabilities. 2013; 34(11):3875-83. [PMID]
- Godamunne P, Liyanage C, Wimaladharmasooriya N, Pathmeswaran A, Wickremasinghe AR, Patterson C, et al. Comparison of performance of Sri Lankan and US children on cognitive and motor scales of the Bayley scales of infant development. BMC Research Notes. 2014; 7:300. [DOI:10.1186/1756-0500-7-300] [PMID] [PMCID]
- Moore T, Johnson S, Haider S, Hennessy E, Marlow N. Relationship between test scores using the second and third editions of the Bayley Scales in extremely preterm children. The Journal of Pediatrics. 2012; 160(4):553-8. [DOI:10.1016/j.jpeds.2011.09.047] [PMID]
- IRAN Statistical Center. [Iran-statistical-yearbook (Persian)]. Tehran: IRAN Statistical Center; 2020. [Link]
- Azari N, Soleimani F, Vameghi R, Sajedi F, Shahshahani S, Karimi H, et al. A psychometric study of the bayley scales of infant and toddler development in Persian Language Children. Iranian Journal of Child Neurology. 2017; 11(1):50-6. [DOI:10.22037/ijcn.v11i1.12056]
- Pena ED, Spaulding TJ, Plante E. The composition of normative groups and diagnostic decision making: Shooting ourselves in the foot. American Journal of Speech-Language Pathology. 2006; 15(3):247-54. [DOI:10.1044/1058-0360(2006/023)]
- Johnson S, Moore T, Marlow N. Using the Bayley-III to assess neurodevelopmental delay: which cut-off should be used? Pediatric Research. 2014; 75(5):670-4. [PMID]
- Anderson PJ, De Luca CR, Hutchinson E, Roberts G, Doyle LW; Victorian Infant Collaborative Group. Underestimation of developmental delay by the new Bayley-III Scale. Archives of Pediatrics & Adolescent Medicine. 2010; 164(4):352-6. [DOI:10.1001/archpediatrics.2010.20] [PMID]
- Steenis LJ, Verhoeven M, Hessen DJ, van Baar AL. Performance of Dutch Children on the Bayley III: A comparison study of US and Dutch Norms. PLoS One. 2015; 10(8):e0132871. [DOI:10.1371/journal.pone.0132871] [PMID] [PMCID]
Type of Study: Original |
Subject:
Pediatric Neurology
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
