

Volume 25, Issue 2 (Summer 2024)
jrehab 2024, 25(2): 312-335 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Lotfi Y, Parhizgar M, Doosti A, Bakhshi E. Investigating the Effects of Pitch Discrimination-based Rehabilitation on Indices and Results of Diagnostic Tests of Children Suspected of Auditory Processing Disorder. jrehab 2024; 25 (2) :312-335
URL: http://rehabilitationj.uswr.ac.ir/article-1-3341-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3341-en.html



1- Department of Audiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Audiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,mohammadrezaparhizgar@yahoo.com
3- Department of Audiology, Rehabilitation Sciences Research Center, School of Rehabilitation Sciences, Shiraz University of Medical Sciences, Shiraz, Iran.
4- Department of Biostatistics and Epidemiology, School of Social Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Audiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
3- Department of Audiology, Rehabilitation Sciences Research Center, School of Rehabilitation Sciences, Shiraz University of Medical Sciences, Shiraz, Iran.
4- Department of Biostatistics and Epidemiology, School of Social Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 3996 kb]
(1232 Downloads)
| Abstract (HTML) (5608 Views)
Full-Text: (1601 Views)
Introduction
According to the definition of the American Speech-Language-Hearing Association (ASHA), auditory processing disorder (APD) is a heterogamous problem resulting from different auditory processing deficits, such as hearing discrimination, auditory pattern recognition, temporal aspects of sounds, and hearing ability in the presence of competing acoustic signals [1]. It leads to various symptoms and complaints in affected populations [2]. In their report on several deficits in extracting auditory messages and other problems, Chalfant and Scheffelin (1969) referred to disorders in perceiving the suprasegmental features of speech and musical aspects of sounds, like pitch, rhythm, and melody [3]. Children with APD are unable to perceive pitches and simulate tunes or detect structural deviation of tunes despite their normal auditory thresholds [4].
Pitch is the perceptual manifestation of sound frequencies and is defined as a perceptual signal that can classify sounds on a bottom-up scale [5]. However, despite their normal hearing, children with APD cannot perceive pitches, simulate tunes, or detect the structural deviations of tunes [4]. Findings have confirmed the poor pitch perceptions of children with APD. Nevertheless, employing efficient approaches to enhancing pitch discrimination and perception ability has been fruitful in various functional domains of these children [6]. Micheyl et al. [7] showed that pitch discrimination-based training positively impacted speech perception in the presence of background noises and significantly improved samples’ tone detection in the presence of noise.
Pitch discrimination-based rehabilitative approaches have yielded positive outcomes, even in the presence of noise, in many cases, for example, by using hearing aids or cochlear implants [6, 7]. Hence, pitch discrimination improvement in children with APD, especially in cases with pitch discrimination deficits, may strengthen children’s perceptions of verbal subsets in the presence of noise and pitch patterns. An assessment of these abilities is one aspect of APD diagnostic signs. Can pitch discrimination improvement change the diagnostic results of APD tests? At present, there are the two following test sets to evaluate and diagnose APD in children [8]: The screening test for auditory processing disorder and the multiple auditory processing assessment (MAPA).
The purposes of these test sets are the early discovery and detection of APD in children for timely interventions [9].
In an attempt to prepare a valid behavioral test, Domitz and Schow presented a set of APD tests for school-age children, i.e. MAPA, which included five subsets in three auditory processing domains [9] as follows: Temporal, monaural, and binaural.
Pitch pattern sequence (PPS) and tap tests are in the temporal domain, and the monaural selective auditory attention test (mSAAT) examines monaural processing. Also, the dichotic digit test (DDT) and competing sentence tests are used for dichotic assessments.
Following different investigations, ASHA (2005) showed that a single test with three standard deviations or two tests with two standard deviations below the mean were suitable for APD diagnosis [1]. However, we will act based on the guidelines of the American Academy of Audiology (AAA) in 2010, suggesting two or more standard deviations below the mean, minimally for one ear, in two different central behavioral tests for APD diagnosis [10]. During the diagnostic process, we administered a subtest of every auditory processing domain, selected the needed samples, and entered them into the study by considering ASHA guidelines (2010) and benefiting from a valid questionnaire.
Although numerous auditory processing tests have been designed and formulated, the monaural selective auditory attention, pitch pattern, and dichotic digit tests have manifested a sensitivity of 90% and specificity of 100% for APD diagnosis [8].
Accordingly, by compiling a rehabilitative program based on pitch discrimination in APD-suspected children with pitch discrimination deficits according to MAPA guidelines and DDT, mSAAT, and pitch pattern test (PPT), we examine the effect of this rehabilitative process on the diagnostic indices of these tests.
Materials and Methods
This study was designed in the Audiology Department of the University of Social Welfare and Rehabilitation Sciences and approved by the secretary of the university/regional research Ethics Committee and performed from 2018 to 2020 on students of Shiraz City, Iran, in collaboration with the Fars Province Department of Education. The entire process was explained to the parents before any intervention, and written consent was obtained from them.
Study participants
All children were selected from primary school students in Shiraz City, Iran. As there was no norm for pitch discrimination in children of the same age, a pilot study was conducted to obtain the range of pitch discrimination in children with normal hearing based on previous research under the supervision of a statistical consultant. Accordingly, 38 male and 37 female participants at a mean age of 10.59±1.42 years were selected for this study. All children were within the normal range regarding hearing and APD assessments. The norm data of pitch discrimination were obtained through this assessment, which was considered a criterion for children with APD to enter rehabilitation sessions.
In the trial phase, 19 children at a mean age of 9.87±0.820 years participated in the experimental group. Of these participants, 7 were female (37%) and 12(63%) were male. The control group consisted of 26 children at a mean age of 9.58±0.705 years, including 15 males (58%) and 11(42%) females.
Auditory processing disorder assessments
Indicators
The inclusion criteria for all children in the study included the following items: Pure tone and speech perception thresholds in audiometric evaluations of 15 dB or less at frequencies between 250 and 8000 Hz in both ears and a speech discrimination (perception) score of at least 92% for both ears; normal function of the middle ear (tympanogram type A); intelligence score of 85 or higher in the Persian version of the Leiter test; Persian monolingual children with Persian monolingual parents; right-hand dominant; no history of academic music education; no history of attention deficit hyperactivity disorder, epilepsy, behavioral and developmental disorders, as well as no history of any medical intervention and central nervous system problems.
Special indicators were considered for children suspected of auditory processing disorders encompass. In addition to pure tone thresholds and speech comprehension in audiometric assessments, with a level of 15 dB or lower within the frequency range of 250 to 8000 Hz and a speech discrimination score of at least 92% for both ears, children with auditory processing disorders typically encounter challenges in understanding amidst noise; conversely, deficient speech discrimination in quiet conditions may indicate neurological damage [10]in addition to the aforementioned criteria and the following items: Weakness of at least two standard deviations for at least one ear in a minimum of two subsets of tests from the multiple assessment set of auditory processing [9] and the pitch discrimination threshold of at least two standard deviations higher than the norm values, with a significance level of P>0.95, for all four notes evaluated in the research.
Before the study, normal data for the PPS test were obtained from 139 children aged 8 to 12 years (76 females and 63 males). The criteria of mSAAT, DDT, and speech in noise tests were also the data obtained from the studies conducted on the Persian versions of these tests [11-13].
Monaural selective auditory attention test (mSAAT)
mSAAT has been selected from the monaural diagnostic tests of MAPA. Monaural selective auditory attention is a monaural low-redundancy test used to measure selective attention skills in children. A child with poor performance in this test can be expected to experience difficulties in discriminating speech in the presence of noise or open background voices.
This test comprises two 25-word lists presented by a similar speaker in the presence of a competing story at a signal-to-noise Ratio of 0 dB [14]. The Persian version of this test with a content validity index of 0.88 is suitably valid for assessing selective attention auditory skills. The test was performed at the 50 dB HL level separately for every ear based on the presented guidelines in the main reference. Speech discrimination tests are performed in the presence of noise or background sounds to probe auditory closure processing and are specifically sensitive to deficits in the brain stem with the auditory cortex [15]. This test is scored based on the child’s correct responses to a 25-item list.
Dichotic digit test
Such test sets target binaural integration processing and are sensitive to deficiencies in the brain stem, cerebral cortex, and corpus callosum [15]. Musiek (1983) examined this test, during which two monosyllabic digit pairs (one to ten in English, except seven) are presented to both ears simultaneously [16]. Two digits are presented to every ear, and ordinal numbers are heard by two ears at the same time, and the person should repeat all four digits within 5 s after their presentation. This method of assessment was first introduced by Broadbent in 1954 [17]. Digits are presented with a pressure of 50 dB above the sensation level, and the interval between each digit pair is 0.5 s.
The Persian version of this test, presented in 2005, is administered with Persian digits (1 to 10, except for 4) [18]. This version was standardized in 2016 for 8-12-year-old children [12]. In this study, we presented digits at the 50 dB sensation level regarding the speech perception threshold, and the child should repeat all four digits. The list included 80 digits, i.e. four per ear. We estimated the total score of each ear by considering the number of the stated correct numbers and assigning a 2.5% point per word.
Pitch pattern test
When discussing pitch discrimination-based rehabilitation, we should access a pitch performance background in auditory processing. Pitch as a tool examining the auditory processing power has been privileged since 1977 [19]. It is a subset of temporal pattern tests of the auditory processing system [20] and is specifically sensitive to cortical lesions and inter-hemisphere relations [15]. PPT is one of the most conventional auditory processing tests [21] and includes three consecutive tones, where the frequency of one is different from the other two [22].
This test was designed for the examination of auditory complications derived from brain lesions [23]. Children’s PPT performance is strongly influenced by timing guidelines, the number of stimuli, and the response type needed [24]. In addition, the perception of these auditory patterns is impacted by the acoustic characteristics of the stimulus, attention, working memory, and experience [25]. The child version of this test includes 30 triad tones of either pitch (880 Hz or 1430 Hz). The duration and the rising/falling time of every tone presented at the 50 dB HL are 500 ms and 10 ms. The interval between two consecutive tones is 300 ms, and the interval between two series of consecutive stimuli is 10 s [26]. In the adult version, which targets ages above 10, two 880 Hz and 1122 Hz frequencies are employed. The duration and rising/falling time of every tone is 200 ms and 10 ms. The intervals between two tones and two series of stimuli are 150 ms and 6 s, respectively [27]. The presented pressure in our research was 50 dB HL, almost equal to the 70 dB sound pressure level in these frequencies [22]. Thirty triad series are presented to every ear, and the child should explain their pitch patterns. This test is scored based on the number of correctly-articulated series.
Pitch discrimination evaluation
The participants were given two notes, starting 1.2 s apart, to assess the pitch discrimination. The presentation time of each stimulus was 500±50 ms (Figure 1). The sounds were recorded digitally at a sampling rate of 44.1 kHz and a quality of 320 kbps [28]. Sounds were presented using the Beats Studio 2 headphones by Asus Lab Top N43J.

A standby image (?) is displayed for one second before the notes (F#3 and C3) are presented. The duration of each note is 600 ms, which are presented at intervals of 600 ms. After the second note is presented, the child has 5000 ms to respond. The correct response is shown to the child only in the process of rehabilitation.
The piano is the most common musical instrument. Its tones are most frequently used as stimulates in frequency modulation evaluations to the extent that some of the researchers use the “absolute piano” phrase instead of “absolute pitch” [29]. In this study, we also utilized this instrument for pitch discrimination purposes. We also began our rehabilitation with the piano.
Stimulus intensity was adjusted to the sound pressure level of 67-68dB. The provided sounds were in biphasic and simultaneous mode. At the same time as presenting the first note, a red circle with the number 1 inserted in the middle was shown to the children, and at the same time as presenting the second note, a blue square with the number 2 inserted in the middle was shown to them. They were taught to identify the higher note after hearing the second sound. Following the presentation of two notes, the child had 5 s to respond. In case of receiving no response, the respective couple would be removed from the statistical calculations. They could select the desired note by referring to the color, shape, number, or order of the notes. Pairs were presented randomly, and evaluations started from an octave distance. Similar research suggests that the rate of pitch discrimination in individuals without any musical training is less than one octave (Figure 2) [30].
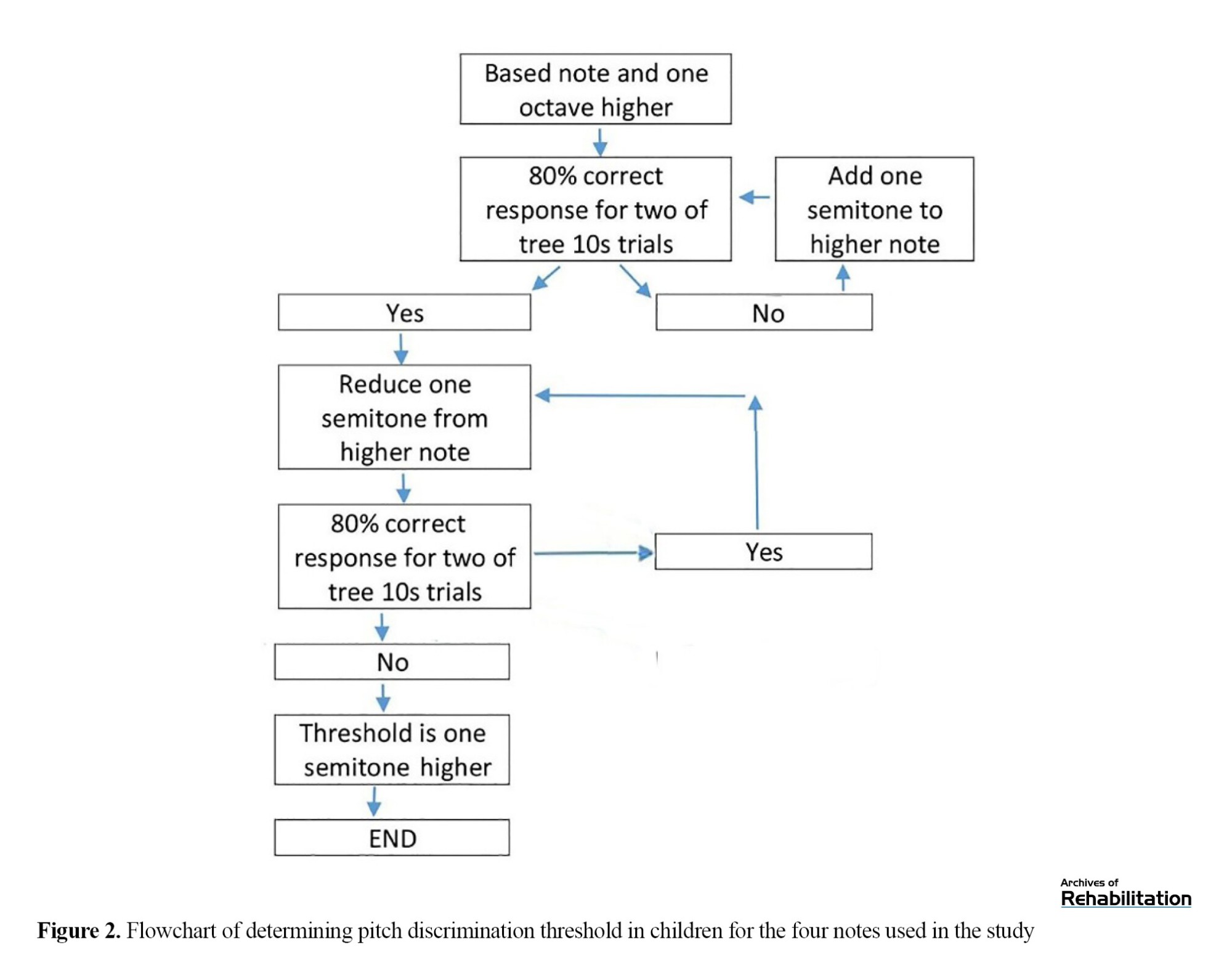
The minimum distance threshold is based on semitone, the level at which children can answer two sets of ten (out of three sets) correctly at a rate of at least %80 (P=0.05). This criterion is not available by diminishing the distance of one semitone.
Thresholds were rated for four notes as follows: [F#3] at 185 Hz, [C4] at 262 Hz, [E4] at 330 Hz, and [G4] at 391 Hz. These sets of notes were designed digitally with a uniform temporal envelope based on the middle note of piano C (262 Hz), and the octave surrounding middle C is the most common octave among the prototypical frequency ranges for Western musical instruments and sung voice [31].
Rehabilitation process
A semitone below the threshold was used for thresholds below one octave to perform rehabilitation. An octave below the threshold was used for cases above one octave, and thus rehabilitation began.
First, as in the evaluation stage, two notes were sent in a row. After the presentation, the correct answer was determined and shown to the children. This process was repeated up to ten times, and then the next step, i.e. the evaluation of the effect of training, was started.
The impact of the rehabilitation process was examined in the end. In cases of not obtaining 80% of the pitch discrimination, the rehabilitation process was repeated for the same pair of notes, and assessments were performed again. If the assessment were successful, the distance was diminished by one semitone for those below one octave and by one octave for those above one octave. Then, the process was repeated. Rehabilitation sessions lasted 40 min to a maximum of 50 min.
To evaluate the effect of sound Timbre on the discrimination ability, based on the classification of instruments [28, 32] and according to the difficulty of the pitch discrimination of the device [32, 33], the rehabilitation steps were continued using guitar, violin, flute, and keyboard.
Altogether, one 40- to 50-min session for each note of each musical instrument was held, and a total of 20 rehabilitation sessions were held continuously two to a maximum of three sessions per week. These sessions lasted up to three months for each child.
Post-rehabilitation evaluations
The pre-rehabilitation assessments were repeated after the end of the rehabilitation period. After at least another month, these assessments were repeated. The children in the control group were thoroughly re-evaluated three months after the first evaluations.
Statistical methods
The figures represent percentages computed for every test on each ear. The covariance test was used to estimate the pre- and post-rehabilitation outcomes statistically. The Mann-Whitney test was used to compare the results of the pitch discrimination rate after rehabilitation in children with APD and normal values. All analyses were run in the SPSS software, version 22.
Results
This study was conducted on 45 children with APD, including 7 females and 12 males with a mean age of 9.87±0.820 years in the experimental group and 11 females and 15 males with a mean age of 9.58±0.705 years in the control group. The Shapiro-Wilk test showed that the age distribution of control (P=0.716) and test (P=0.987) groups had a normal distribution. The Leven test showed that the age data had equal variance (P=0.938). The independent t-test also showed that the mean age of the two groups did not differ significantly (P=0.158). The chi-square test showed that the ratio of male to female participants was not statistically different (P=0.712).
The pitch discrimination data were compared between the experimental group and normal data using the Mann-Whitney U test. Post-rehabilitation evaluation data showed a significant improvement in the rate of pitch discrimination in the experimental group compared to normal values (P<0.001) (Figure 3).
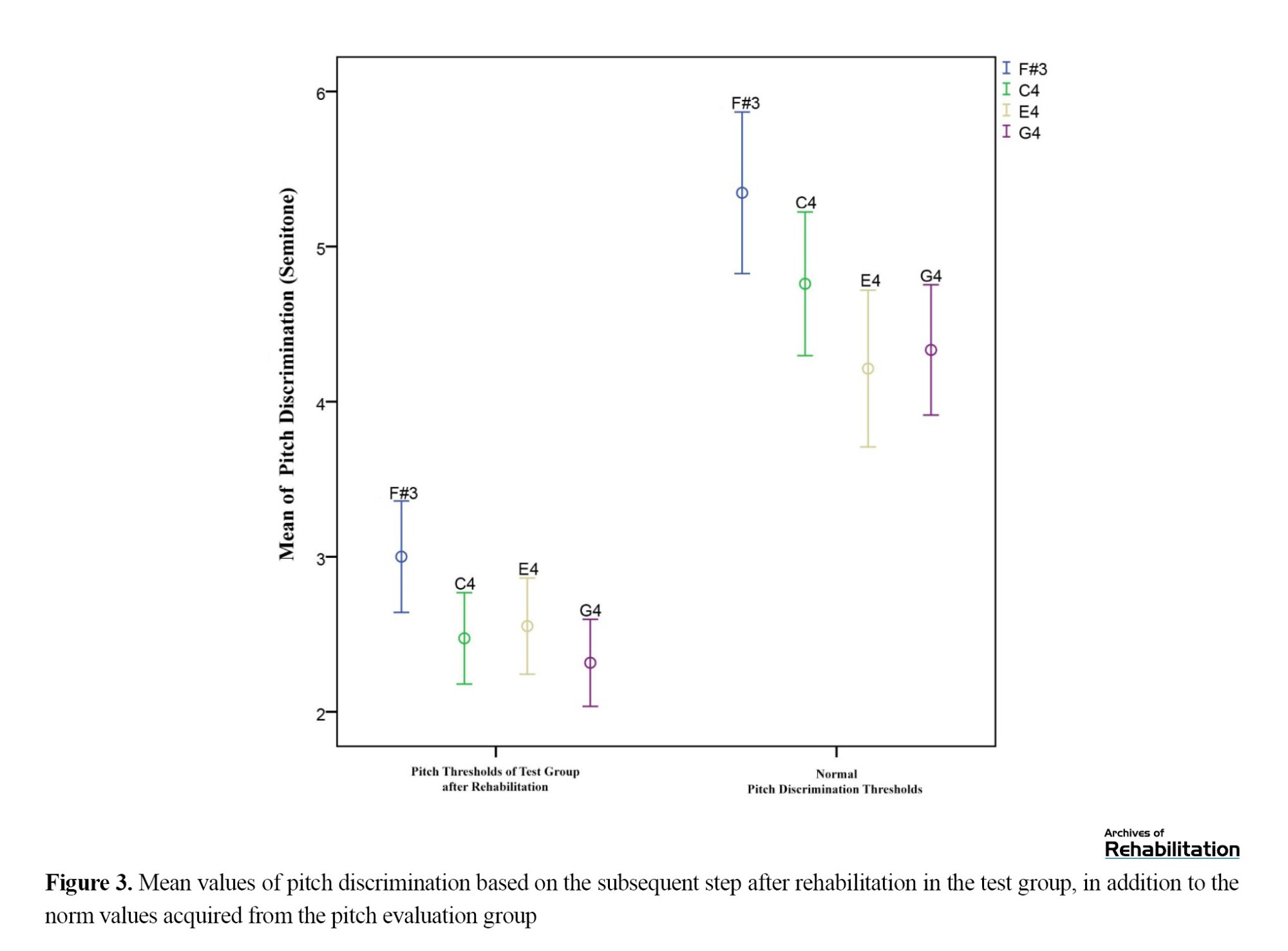
The right-side indicators on the chart (Figure 3) depict the pitch discrimination values obtained for the four notes evaluated in the normative study (75 children). The left-side indicators represent the average pitch discrimination in the children of the test group after the intervention (19 children).
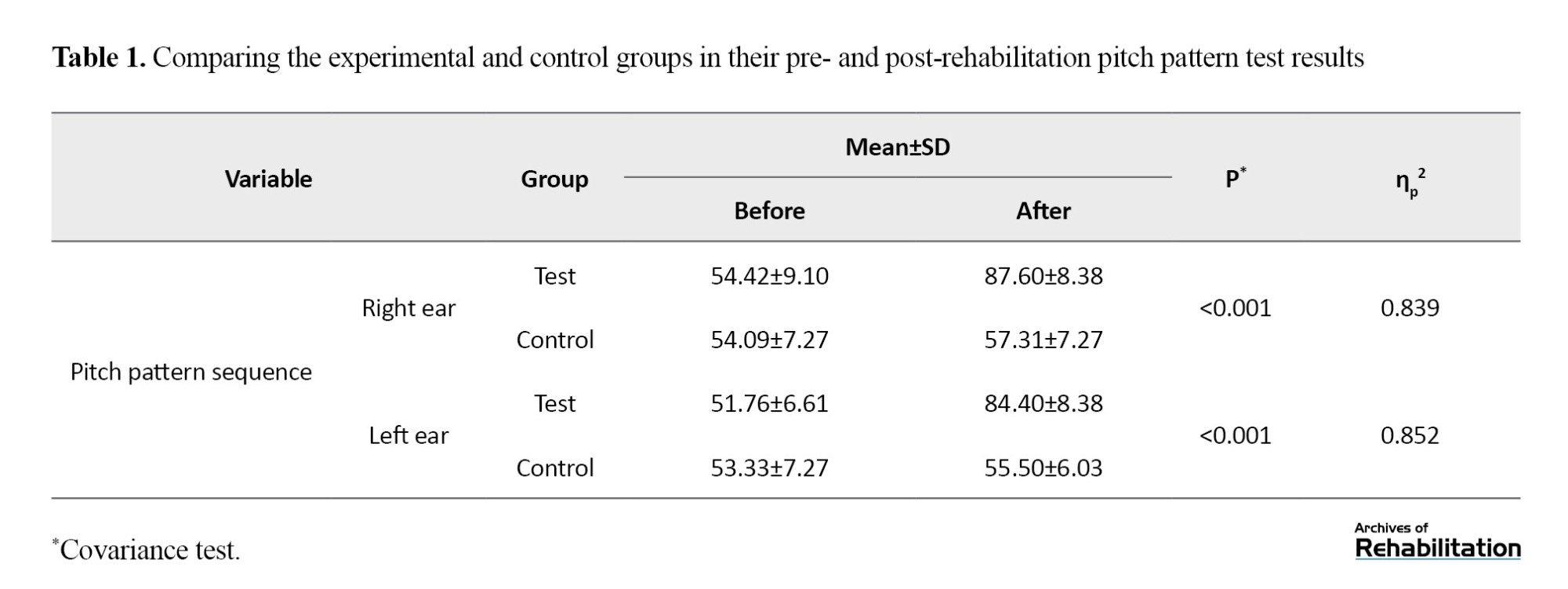
Improvements in children’s pitch discrimination capacity made their PPT outperformance (Table 1) more expected, which was realized based on estimations.
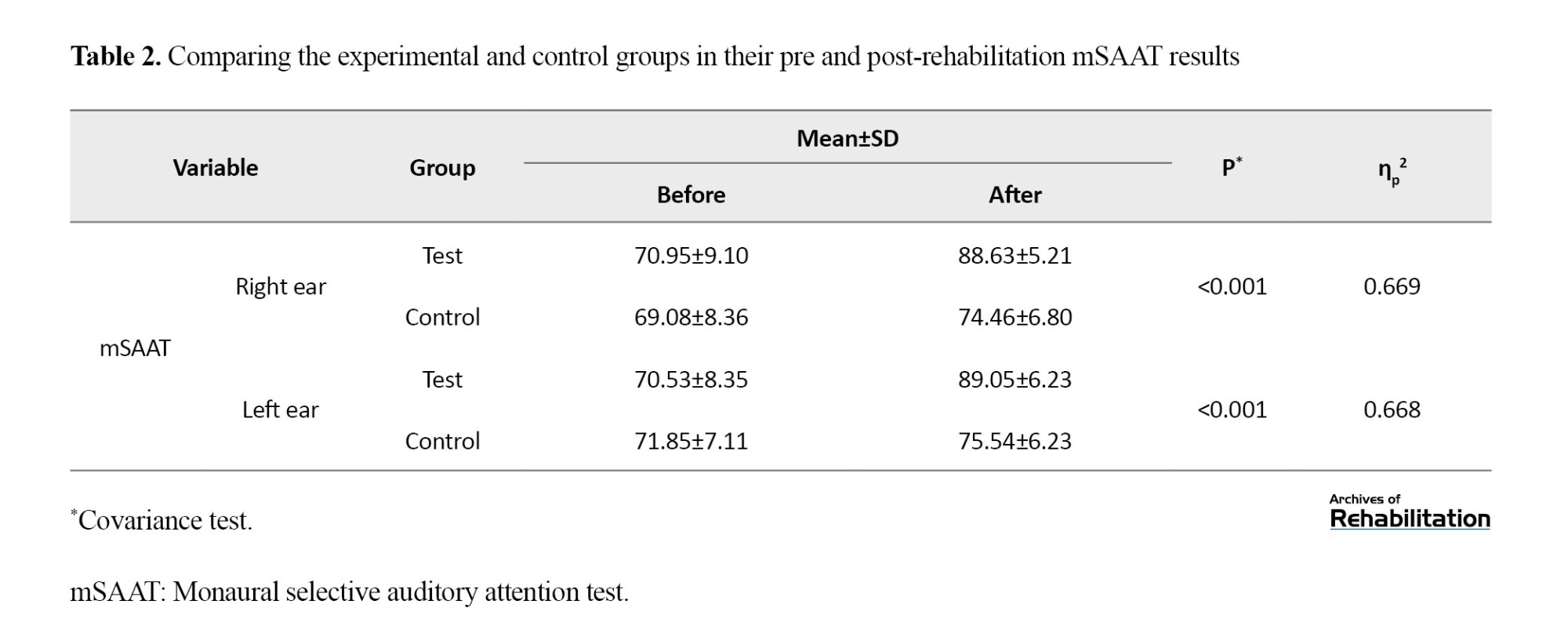
However, another aspect of the assessment included the mSAAT test, i.e. discriminating verbal concepts in the presence of a background speech. mSAAT is a type of speech perception test administered in the presence of background noise. The assessment indicated significant improvement in speech discrimination in the presence of background noise after the effective process of pitch discrimination-based rehabilitation (Table 2).
The last test of this series was DDT, which is subsumed under binaural tests and requires the child to process every ear’s stimulant separately and retrieve the different speeches of two ears. The statistical analysis of the results before and after the pitch discrimination-based rehabilitation illustrated no statistical improvement in this test set (Table 3).

Discussion
The effects of pitch discrimination-based rehabilitation on pitch pattern test results
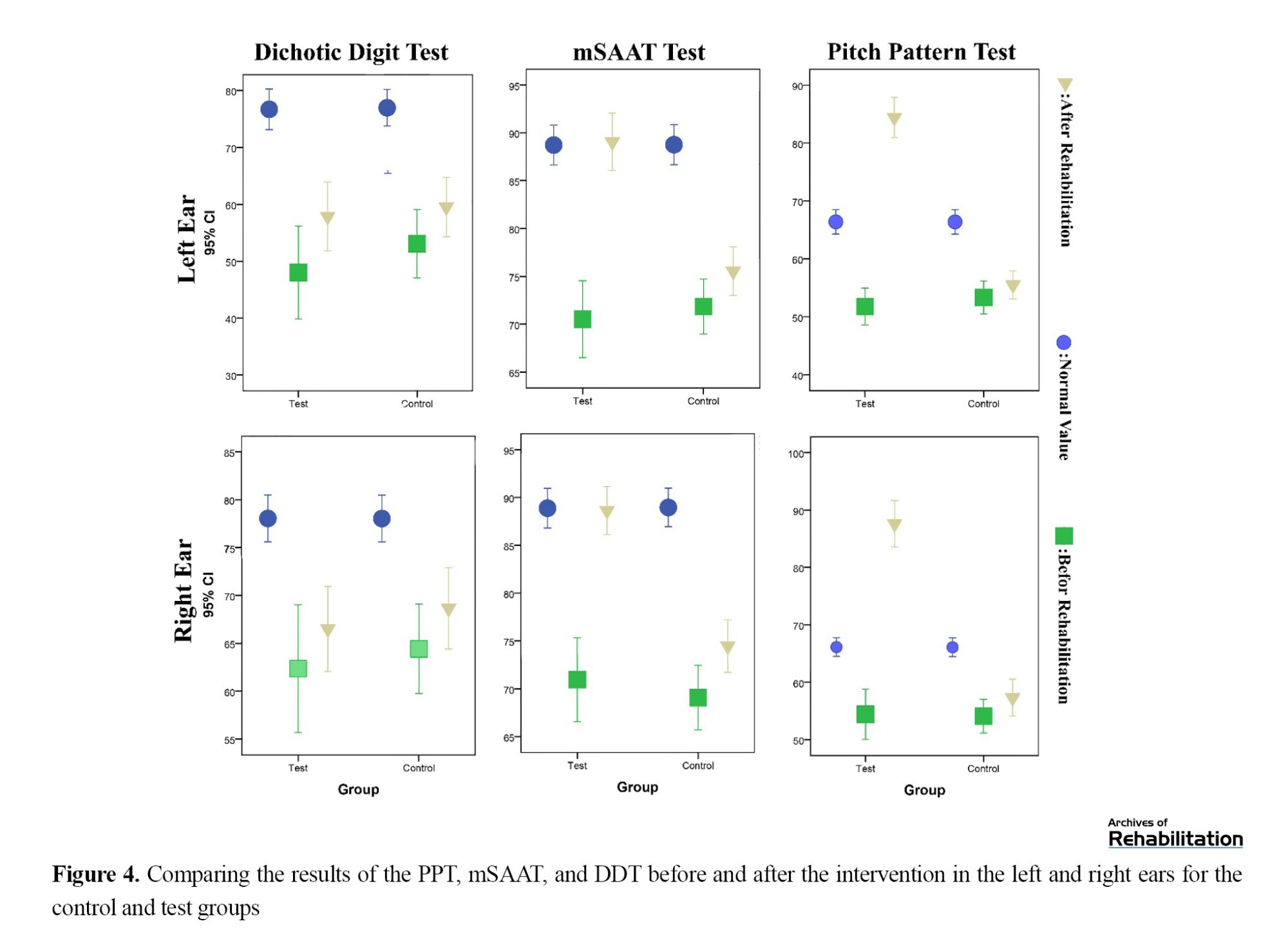
In a systematic study, Apfelstadt (1984) examined the effects of melodic perception training on pitch discrimination and discovered no signs of pitch discrimination improvement in samples. However, the training led to explicit and significant improvement in pitch pattern singing [34]. Table 1 demonstrates that the intervention and rehabilitative process has positively and directly influenced PPT outcomes in children with APD. The children’s ears were positively impacted by the rehabilitation and showed significant improvements (P<0.001). The PPT scores of all intervened children fell into or above the estimated normal range (Figure 4). Hence, the first achievement of the pitch discrimination-based intervention was eliminating one of the APD indices in these children. Accordingly, many of these children did not manifest an index of APD in any of their ears after pitch discrimination-based rehabilitation.
The effect of pitch discrimination-based rehabilitation on the monaural selective auditory attention test outcomes
According to Table 2, the discrimination percentage of mSAAT has significantly improved after the rehabilitation (P<0.001). As previously mentioned, this test comprises 25-word lists expressed by the speaker in the presence of a competing story in the signal-to-noise ratio of 0 dB [14]. The presence of a similar speaker as a background and confounding noise and the target speech can engender a dual challenge for speech discrimination in the presence of background noise: First, similar to other tests, the child should discriminate the target speech from the background speech, and, second, both speeches are presented by a single speaker with a base sound pattern.
One of the theories that rationalize the enhancement in musicians’ speech comprehension amid noise is perceptual anchoring [35]. Perceptual anchoring denotes internal and consistent capabilities that develop in response to repetitive stimuli. For example, in tasks involving frequency discrimination, maintaining an unaltered reference tone yields superior thresholds in comparison to a continuously changing reference tone [36]. An argument advocating the advantage of perceptual anchoring posits that a stable reference tone contributes to the cultivation of heightened perceptual stability, facilitating the detection of the test tone and consequently refining perceptual discrimination [37]. The ability to establish perceptual anchoring in the speaker’s speech, augmenting pitch discrimination, is deemed pivotal for ameliorating the understanding of the target signal amidst background noise [38]. After the amelioration in pitch discrimination resulting from rehabilitation in children, this phenomenon can streamline the tracking of a stable and specific target sound amid background noise, leading to an augmentation in their speech comprehension scores.
Sares (2017) investigated the relationships of pitch processing and time with tonal stimuli and speech and specifically referred to the link between attention and pitch and temporal discrimination capacities. This research argued that musicianship could not be directly associated with attention by itself; rather, music-tied training could impact direct and indirect attention positively [39]. Thus, we conclude that pitch discrimination training can raise and improve the child’s attention and concentration in the auditory process. This attentional improvement can pave the way for speech perception in mSSAT in the presence of noise. As a result of this intervention, the right-ear mSAAT results of almost 37% of children with deficits more than two standard deviations from normal values did not fall into this range, and the left-ear results of about 78% of similar cases were also not in the described deficiency range.
Hence, the rehabilitative benefits and pitch discrimination improvements can influence mSAAT results and increase its score due to the raised attention derived from pitch discrimination rehabilitation (Figure 4).
The effect of pitch discrimination-based rehabilitation on dichotic digit test results
Following two effective outcomes of the pitch discrimination-based rehabilitation in the PPT and mSAAT tests, we found no impact of this intervention on the DDT results (Table 3). Accordingly, the pitch discrimination-based rehabilitation brought about significant improvement in the DDT outcomes neither for the right (P=0.643) nor for the left ear (P=0.239).
The justification for this finding is the separate processing paths of these two sets, i.e. pitch discrimination and DDT tests follow two different processing paths in the auditory system. As previously mentioned, DDT is sensitive to deficiencies in the brain stem, cerebral cortex, and corpus callosum, while PPT is sensitive to cortical lesions and inter-hemisphere relations [15]. Thus, the pitch discrimination path is separate from the dichotic digit processing path, and expecting that pitch discrimination improvements can directly influence individuals’ retrieval of dichotic digits is not supported and rationally accepted (Figure 4).
Pitch discrimination-based rehabilitation and diagnostic auditory processing disorder indices
The comparison of the post-rehabilitation data showed that 7 intervened children (three girls and four boys) were no longer classified into the group of children suspected of APD. None of the seven children manifested a drop of two standard deviations, minimally for one ear, in two administered tests after the pitch discrimination-based rehabilitation. Perhaps, the claim of APD removal in these children is unimaginable; yet, the least achievement of this rehabilitation is that the diagnostic criterion for the presence of APD based on MAPA tests cannot be imagined for about 37%, i.e. over one-third, according to the guidelines of the ASHA (2010) [9]. This means that if these children are assessed by DDT, mSAAT, and PPT tests with a confirmed sensitivity of 90% and specificity of 100% for APD diagnosis [9], they are not classified as APD children according to AAA guidelines if their indices are two standard deviations below the mean, minimally for one ear, in two tests.
Conclusion
Pitch discrimination-based rehabilitation differently impacts MAPA subtests. However, the outcomes revealed salient improvements in some of these tests. The effect of this intervention was to the extent that over one-third of the children suspected of APD were no longer classified into the APD group based on the employed criteria in this research.
Ethical Considerations
Compliance with ethical guidelines
This was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1397.087). Before commencement, all participants were briefed on the study’s stages, objectives, and methodologies. Upon expressing willingness to participate, each participant formally endorsed an informed written consent form. Strict confidentiality of participant information was upheld throughout the study. Additionally, participants were afforded the autonomy to withdraw from the study at any point without the requirement of furnishing a specific reason.
Funding
The present article was extracted from the PhD dissertation of Yones Lotfi, approved by Department of Audiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Conceptualization and methodology: Mohammadreza Parhizgar, Yones Lotfi, Afsaneh Doosti; Visualization, project management, data collection and writing the initial draft: Mohammadreza Parhizgar; Data analysis: Mohammadreza Parhizgar and Enayatollah Bakhshi; Review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank Saeed Tavanger, at Special Education Organization of Fars Province, Iran.
According to the definition of the American Speech-Language-Hearing Association (ASHA), auditory processing disorder (APD) is a heterogamous problem resulting from different auditory processing deficits, such as hearing discrimination, auditory pattern recognition, temporal aspects of sounds, and hearing ability in the presence of competing acoustic signals [1]. It leads to various symptoms and complaints in affected populations [2]. In their report on several deficits in extracting auditory messages and other problems, Chalfant and Scheffelin (1969) referred to disorders in perceiving the suprasegmental features of speech and musical aspects of sounds, like pitch, rhythm, and melody [3]. Children with APD are unable to perceive pitches and simulate tunes or detect structural deviation of tunes despite their normal auditory thresholds [4].
Pitch is the perceptual manifestation of sound frequencies and is defined as a perceptual signal that can classify sounds on a bottom-up scale [5]. However, despite their normal hearing, children with APD cannot perceive pitches, simulate tunes, or detect the structural deviations of tunes [4]. Findings have confirmed the poor pitch perceptions of children with APD. Nevertheless, employing efficient approaches to enhancing pitch discrimination and perception ability has been fruitful in various functional domains of these children [6]. Micheyl et al. [7] showed that pitch discrimination-based training positively impacted speech perception in the presence of background noises and significantly improved samples’ tone detection in the presence of noise.
Pitch discrimination-based rehabilitative approaches have yielded positive outcomes, even in the presence of noise, in many cases, for example, by using hearing aids or cochlear implants [6, 7]. Hence, pitch discrimination improvement in children with APD, especially in cases with pitch discrimination deficits, may strengthen children’s perceptions of verbal subsets in the presence of noise and pitch patterns. An assessment of these abilities is one aspect of APD diagnostic signs. Can pitch discrimination improvement change the diagnostic results of APD tests? At present, there are the two following test sets to evaluate and diagnose APD in children [8]: The screening test for auditory processing disorder and the multiple auditory processing assessment (MAPA).
The purposes of these test sets are the early discovery and detection of APD in children for timely interventions [9].
In an attempt to prepare a valid behavioral test, Domitz and Schow presented a set of APD tests for school-age children, i.e. MAPA, which included five subsets in three auditory processing domains [9] as follows: Temporal, monaural, and binaural.
Pitch pattern sequence (PPS) and tap tests are in the temporal domain, and the monaural selective auditory attention test (mSAAT) examines monaural processing. Also, the dichotic digit test (DDT) and competing sentence tests are used for dichotic assessments.
Following different investigations, ASHA (2005) showed that a single test with three standard deviations or two tests with two standard deviations below the mean were suitable for APD diagnosis [1]. However, we will act based on the guidelines of the American Academy of Audiology (AAA) in 2010, suggesting two or more standard deviations below the mean, minimally for one ear, in two different central behavioral tests for APD diagnosis [10]. During the diagnostic process, we administered a subtest of every auditory processing domain, selected the needed samples, and entered them into the study by considering ASHA guidelines (2010) and benefiting from a valid questionnaire.
Although numerous auditory processing tests have been designed and formulated, the monaural selective auditory attention, pitch pattern, and dichotic digit tests have manifested a sensitivity of 90% and specificity of 100% for APD diagnosis [8].
Accordingly, by compiling a rehabilitative program based on pitch discrimination in APD-suspected children with pitch discrimination deficits according to MAPA guidelines and DDT, mSAAT, and pitch pattern test (PPT), we examine the effect of this rehabilitative process on the diagnostic indices of these tests.
Materials and Methods
This study was designed in the Audiology Department of the University of Social Welfare and Rehabilitation Sciences and approved by the secretary of the university/regional research Ethics Committee and performed from 2018 to 2020 on students of Shiraz City, Iran, in collaboration with the Fars Province Department of Education. The entire process was explained to the parents before any intervention, and written consent was obtained from them.
Study participants
All children were selected from primary school students in Shiraz City, Iran. As there was no norm for pitch discrimination in children of the same age, a pilot study was conducted to obtain the range of pitch discrimination in children with normal hearing based on previous research under the supervision of a statistical consultant. Accordingly, 38 male and 37 female participants at a mean age of 10.59±1.42 years were selected for this study. All children were within the normal range regarding hearing and APD assessments. The norm data of pitch discrimination were obtained through this assessment, which was considered a criterion for children with APD to enter rehabilitation sessions.
In the trial phase, 19 children at a mean age of 9.87±0.820 years participated in the experimental group. Of these participants, 7 were female (37%) and 12(63%) were male. The control group consisted of 26 children at a mean age of 9.58±0.705 years, including 15 males (58%) and 11(42%) females.
Auditory processing disorder assessments
Indicators
The inclusion criteria for all children in the study included the following items: Pure tone and speech perception thresholds in audiometric evaluations of 15 dB or less at frequencies between 250 and 8000 Hz in both ears and a speech discrimination (perception) score of at least 92% for both ears; normal function of the middle ear (tympanogram type A); intelligence score of 85 or higher in the Persian version of the Leiter test; Persian monolingual children with Persian monolingual parents; right-hand dominant; no history of academic music education; no history of attention deficit hyperactivity disorder, epilepsy, behavioral and developmental disorders, as well as no history of any medical intervention and central nervous system problems.
Special indicators were considered for children suspected of auditory processing disorders encompass. In addition to pure tone thresholds and speech comprehension in audiometric assessments, with a level of 15 dB or lower within the frequency range of 250 to 8000 Hz and a speech discrimination score of at least 92% for both ears, children with auditory processing disorders typically encounter challenges in understanding amidst noise; conversely, deficient speech discrimination in quiet conditions may indicate neurological damage [10]in addition to the aforementioned criteria and the following items: Weakness of at least two standard deviations for at least one ear in a minimum of two subsets of tests from the multiple assessment set of auditory processing [9] and the pitch discrimination threshold of at least two standard deviations higher than the norm values, with a significance level of P>0.95, for all four notes evaluated in the research.
Before the study, normal data for the PPS test were obtained from 139 children aged 8 to 12 years (76 females and 63 males). The criteria of mSAAT, DDT, and speech in noise tests were also the data obtained from the studies conducted on the Persian versions of these tests [11-13].
Monaural selective auditory attention test (mSAAT)
mSAAT has been selected from the monaural diagnostic tests of MAPA. Monaural selective auditory attention is a monaural low-redundancy test used to measure selective attention skills in children. A child with poor performance in this test can be expected to experience difficulties in discriminating speech in the presence of noise or open background voices.
This test comprises two 25-word lists presented by a similar speaker in the presence of a competing story at a signal-to-noise Ratio of 0 dB [14]. The Persian version of this test with a content validity index of 0.88 is suitably valid for assessing selective attention auditory skills. The test was performed at the 50 dB HL level separately for every ear based on the presented guidelines in the main reference. Speech discrimination tests are performed in the presence of noise or background sounds to probe auditory closure processing and are specifically sensitive to deficits in the brain stem with the auditory cortex [15]. This test is scored based on the child’s correct responses to a 25-item list.
Dichotic digit test
Such test sets target binaural integration processing and are sensitive to deficiencies in the brain stem, cerebral cortex, and corpus callosum [15]. Musiek (1983) examined this test, during which two monosyllabic digit pairs (one to ten in English, except seven) are presented to both ears simultaneously [16]. Two digits are presented to every ear, and ordinal numbers are heard by two ears at the same time, and the person should repeat all four digits within 5 s after their presentation. This method of assessment was first introduced by Broadbent in 1954 [17]. Digits are presented with a pressure of 50 dB above the sensation level, and the interval between each digit pair is 0.5 s.
The Persian version of this test, presented in 2005, is administered with Persian digits (1 to 10, except for 4) [18]. This version was standardized in 2016 for 8-12-year-old children [12]. In this study, we presented digits at the 50 dB sensation level regarding the speech perception threshold, and the child should repeat all four digits. The list included 80 digits, i.e. four per ear. We estimated the total score of each ear by considering the number of the stated correct numbers and assigning a 2.5% point per word.
Pitch pattern test
When discussing pitch discrimination-based rehabilitation, we should access a pitch performance background in auditory processing. Pitch as a tool examining the auditory processing power has been privileged since 1977 [19]. It is a subset of temporal pattern tests of the auditory processing system [20] and is specifically sensitive to cortical lesions and inter-hemisphere relations [15]. PPT is one of the most conventional auditory processing tests [21] and includes three consecutive tones, where the frequency of one is different from the other two [22].
This test was designed for the examination of auditory complications derived from brain lesions [23]. Children’s PPT performance is strongly influenced by timing guidelines, the number of stimuli, and the response type needed [24]. In addition, the perception of these auditory patterns is impacted by the acoustic characteristics of the stimulus, attention, working memory, and experience [25]. The child version of this test includes 30 triad tones of either pitch (880 Hz or 1430 Hz). The duration and the rising/falling time of every tone presented at the 50 dB HL are 500 ms and 10 ms. The interval between two consecutive tones is 300 ms, and the interval between two series of consecutive stimuli is 10 s [26]. In the adult version, which targets ages above 10, two 880 Hz and 1122 Hz frequencies are employed. The duration and rising/falling time of every tone is 200 ms and 10 ms. The intervals between two tones and two series of stimuli are 150 ms and 6 s, respectively [27]. The presented pressure in our research was 50 dB HL, almost equal to the 70 dB sound pressure level in these frequencies [22]. Thirty triad series are presented to every ear, and the child should explain their pitch patterns. This test is scored based on the number of correctly-articulated series.
Pitch discrimination evaluation
The participants were given two notes, starting 1.2 s apart, to assess the pitch discrimination. The presentation time of each stimulus was 500±50 ms (Figure 1). The sounds were recorded digitally at a sampling rate of 44.1 kHz and a quality of 320 kbps [28]. Sounds were presented using the Beats Studio 2 headphones by Asus Lab Top N43J.
A standby image (?) is displayed for one second before the notes (F#3 and C3) are presented. The duration of each note is 600 ms, which are presented at intervals of 600 ms. After the second note is presented, the child has 5000 ms to respond. The correct response is shown to the child only in the process of rehabilitation.
The piano is the most common musical instrument. Its tones are most frequently used as stimulates in frequency modulation evaluations to the extent that some of the researchers use the “absolute piano” phrase instead of “absolute pitch” [29]. In this study, we also utilized this instrument for pitch discrimination purposes. We also began our rehabilitation with the piano.
Stimulus intensity was adjusted to the sound pressure level of 67-68dB. The provided sounds were in biphasic and simultaneous mode. At the same time as presenting the first note, a red circle with the number 1 inserted in the middle was shown to the children, and at the same time as presenting the second note, a blue square with the number 2 inserted in the middle was shown to them. They were taught to identify the higher note after hearing the second sound. Following the presentation of two notes, the child had 5 s to respond. In case of receiving no response, the respective couple would be removed from the statistical calculations. They could select the desired note by referring to the color, shape, number, or order of the notes. Pairs were presented randomly, and evaluations started from an octave distance. Similar research suggests that the rate of pitch discrimination in individuals without any musical training is less than one octave (Figure 2) [30].
The minimum distance threshold is based on semitone, the level at which children can answer two sets of ten (out of three sets) correctly at a rate of at least %80 (P=0.05). This criterion is not available by diminishing the distance of one semitone.
Thresholds were rated for four notes as follows: [F#3] at 185 Hz, [C4] at 262 Hz, [E4] at 330 Hz, and [G4] at 391 Hz. These sets of notes were designed digitally with a uniform temporal envelope based on the middle note of piano C (262 Hz), and the octave surrounding middle C is the most common octave among the prototypical frequency ranges for Western musical instruments and sung voice [31].
Rehabilitation process
A semitone below the threshold was used for thresholds below one octave to perform rehabilitation. An octave below the threshold was used for cases above one octave, and thus rehabilitation began.
First, as in the evaluation stage, two notes were sent in a row. After the presentation, the correct answer was determined and shown to the children. This process was repeated up to ten times, and then the next step, i.e. the evaluation of the effect of training, was started.
The impact of the rehabilitation process was examined in the end. In cases of not obtaining 80% of the pitch discrimination, the rehabilitation process was repeated for the same pair of notes, and assessments were performed again. If the assessment were successful, the distance was diminished by one semitone for those below one octave and by one octave for those above one octave. Then, the process was repeated. Rehabilitation sessions lasted 40 min to a maximum of 50 min.
To evaluate the effect of sound Timbre on the discrimination ability, based on the classification of instruments [28, 32] and according to the difficulty of the pitch discrimination of the device [32, 33], the rehabilitation steps were continued using guitar, violin, flute, and keyboard.
Altogether, one 40- to 50-min session for each note of each musical instrument was held, and a total of 20 rehabilitation sessions were held continuously two to a maximum of three sessions per week. These sessions lasted up to three months for each child.
Post-rehabilitation evaluations
The pre-rehabilitation assessments were repeated after the end of the rehabilitation period. After at least another month, these assessments were repeated. The children in the control group were thoroughly re-evaluated three months after the first evaluations.
Statistical methods
The figures represent percentages computed for every test on each ear. The covariance test was used to estimate the pre- and post-rehabilitation outcomes statistically. The Mann-Whitney test was used to compare the results of the pitch discrimination rate after rehabilitation in children with APD and normal values. All analyses were run in the SPSS software, version 22.
Results
This study was conducted on 45 children with APD, including 7 females and 12 males with a mean age of 9.87±0.820 years in the experimental group and 11 females and 15 males with a mean age of 9.58±0.705 years in the control group. The Shapiro-Wilk test showed that the age distribution of control (P=0.716) and test (P=0.987) groups had a normal distribution. The Leven test showed that the age data had equal variance (P=0.938). The independent t-test also showed that the mean age of the two groups did not differ significantly (P=0.158). The chi-square test showed that the ratio of male to female participants was not statistically different (P=0.712).
The pitch discrimination data were compared between the experimental group and normal data using the Mann-Whitney U test. Post-rehabilitation evaluation data showed a significant improvement in the rate of pitch discrimination in the experimental group compared to normal values (P<0.001) (Figure 3).
The right-side indicators on the chart (Figure 3) depict the pitch discrimination values obtained for the four notes evaluated in the normative study (75 children). The left-side indicators represent the average pitch discrimination in the children of the test group after the intervention (19 children).
Improvements in children’s pitch discrimination capacity made their PPT outperformance (Table 1) more expected, which was realized based on estimations.
However, another aspect of the assessment included the mSAAT test, i.e. discriminating verbal concepts in the presence of a background speech. mSAAT is a type of speech perception test administered in the presence of background noise. The assessment indicated significant improvement in speech discrimination in the presence of background noise after the effective process of pitch discrimination-based rehabilitation (Table 2).
The last test of this series was DDT, which is subsumed under binaural tests and requires the child to process every ear’s stimulant separately and retrieve the different speeches of two ears. The statistical analysis of the results before and after the pitch discrimination-based rehabilitation illustrated no statistical improvement in this test set (Table 3).
Discussion
The effects of pitch discrimination-based rehabilitation on pitch pattern test results
In a systematic study, Apfelstadt (1984) examined the effects of melodic perception training on pitch discrimination and discovered no signs of pitch discrimination improvement in samples. However, the training led to explicit and significant improvement in pitch pattern singing [34]. Table 1 demonstrates that the intervention and rehabilitative process has positively and directly influenced PPT outcomes in children with APD. The children’s ears were positively impacted by the rehabilitation and showed significant improvements (P<0.001). The PPT scores of all intervened children fell into or above the estimated normal range (Figure 4). Hence, the first achievement of the pitch discrimination-based intervention was eliminating one of the APD indices in these children. Accordingly, many of these children did not manifest an index of APD in any of their ears after pitch discrimination-based rehabilitation.
The effect of pitch discrimination-based rehabilitation on the monaural selective auditory attention test outcomes
According to Table 2, the discrimination percentage of mSAAT has significantly improved after the rehabilitation (P<0.001). As previously mentioned, this test comprises 25-word lists expressed by the speaker in the presence of a competing story in the signal-to-noise ratio of 0 dB [14]. The presence of a similar speaker as a background and confounding noise and the target speech can engender a dual challenge for speech discrimination in the presence of background noise: First, similar to other tests, the child should discriminate the target speech from the background speech, and, second, both speeches are presented by a single speaker with a base sound pattern.
One of the theories that rationalize the enhancement in musicians’ speech comprehension amid noise is perceptual anchoring [35]. Perceptual anchoring denotes internal and consistent capabilities that develop in response to repetitive stimuli. For example, in tasks involving frequency discrimination, maintaining an unaltered reference tone yields superior thresholds in comparison to a continuously changing reference tone [36]. An argument advocating the advantage of perceptual anchoring posits that a stable reference tone contributes to the cultivation of heightened perceptual stability, facilitating the detection of the test tone and consequently refining perceptual discrimination [37]. The ability to establish perceptual anchoring in the speaker’s speech, augmenting pitch discrimination, is deemed pivotal for ameliorating the understanding of the target signal amidst background noise [38]. After the amelioration in pitch discrimination resulting from rehabilitation in children, this phenomenon can streamline the tracking of a stable and specific target sound amid background noise, leading to an augmentation in their speech comprehension scores.
Sares (2017) investigated the relationships of pitch processing and time with tonal stimuli and speech and specifically referred to the link between attention and pitch and temporal discrimination capacities. This research argued that musicianship could not be directly associated with attention by itself; rather, music-tied training could impact direct and indirect attention positively [39]. Thus, we conclude that pitch discrimination training can raise and improve the child’s attention and concentration in the auditory process. This attentional improvement can pave the way for speech perception in mSSAT in the presence of noise. As a result of this intervention, the right-ear mSAAT results of almost 37% of children with deficits more than two standard deviations from normal values did not fall into this range, and the left-ear results of about 78% of similar cases were also not in the described deficiency range.
Hence, the rehabilitative benefits and pitch discrimination improvements can influence mSAAT results and increase its score due to the raised attention derived from pitch discrimination rehabilitation (Figure 4).
The effect of pitch discrimination-based rehabilitation on dichotic digit test results
Following two effective outcomes of the pitch discrimination-based rehabilitation in the PPT and mSAAT tests, we found no impact of this intervention on the DDT results (Table 3). Accordingly, the pitch discrimination-based rehabilitation brought about significant improvement in the DDT outcomes neither for the right (P=0.643) nor for the left ear (P=0.239).
The justification for this finding is the separate processing paths of these two sets, i.e. pitch discrimination and DDT tests follow two different processing paths in the auditory system. As previously mentioned, DDT is sensitive to deficiencies in the brain stem, cerebral cortex, and corpus callosum, while PPT is sensitive to cortical lesions and inter-hemisphere relations [15]. Thus, the pitch discrimination path is separate from the dichotic digit processing path, and expecting that pitch discrimination improvements can directly influence individuals’ retrieval of dichotic digits is not supported and rationally accepted (Figure 4).
Pitch discrimination-based rehabilitation and diagnostic auditory processing disorder indices
The comparison of the post-rehabilitation data showed that 7 intervened children (three girls and four boys) were no longer classified into the group of children suspected of APD. None of the seven children manifested a drop of two standard deviations, minimally for one ear, in two administered tests after the pitch discrimination-based rehabilitation. Perhaps, the claim of APD removal in these children is unimaginable; yet, the least achievement of this rehabilitation is that the diagnostic criterion for the presence of APD based on MAPA tests cannot be imagined for about 37%, i.e. over one-third, according to the guidelines of the ASHA (2010) [9]. This means that if these children are assessed by DDT, mSAAT, and PPT tests with a confirmed sensitivity of 90% and specificity of 100% for APD diagnosis [9], they are not classified as APD children according to AAA guidelines if their indices are two standard deviations below the mean, minimally for one ear, in two tests.
Conclusion
Pitch discrimination-based rehabilitation differently impacts MAPA subtests. However, the outcomes revealed salient improvements in some of these tests. The effect of this intervention was to the extent that over one-third of the children suspected of APD were no longer classified into the APD group based on the employed criteria in this research.
Ethical Considerations
Compliance with ethical guidelines
This was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1397.087). Before commencement, all participants were briefed on the study’s stages, objectives, and methodologies. Upon expressing willingness to participate, each participant formally endorsed an informed written consent form. Strict confidentiality of participant information was upheld throughout the study. Additionally, participants were afforded the autonomy to withdraw from the study at any point without the requirement of furnishing a specific reason.
Funding
The present article was extracted from the PhD dissertation of Yones Lotfi, approved by Department of Audiology, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Conceptualization and methodology: Mohammadreza Parhizgar, Yones Lotfi, Afsaneh Doosti; Visualization, project management, data collection and writing the initial draft: Mohammadreza Parhizgar; Data analysis: Mohammadreza Parhizgar and Enayatollah Bakhshi; Review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank Saeed Tavanger, at Special Education Organization of Fars Province, Iran.
References
- Ptok M. [(Central) auditory processing disorders. Remarks on the ASHA Technical Report (German)]. HNO. 2006; 54(1):6-8. [DOI:10.1007/s00106-005-1334-y] [PMID]
- Moore DR. Auditory processing disorders: Acquisition and treatment. Journal of Communication Disorders. 2007; 40(4):295-304 [DOI:10.1016/j.jcomdis.2007.03.005] [PMID]
- Chalfant JC, Scheffelin MA. Central processing dysfunctions in children: A review of research. New York: U.S. National Institutes of Health; 1970. [Link]
- Braun A, McArdle J, Jones J, Nechaev V, Zalewski C, Brewer C, et al. Tune deafness: Processing melodic errors outside of conscious awareness as reflected by components of the auditory ERP. Plos One. 2008; 3(6):e2349. [DOI:10.1371/journal.pone.0002349] [PMID] [PMCID]
- ANSI. American National Standard: Acoustical Terminology. New York: The Acoustical Society of America; 1994. [Link]
- Aying J. The benefits of music education: An overview of current Neuroscience research. Toronto: The Royal Conservatory of Music; 2014. [Link]
- Micheyl C, Delhommeau K, Perrot X, Oxenham AJ. Influence of musical and psychoacoustical training on pitch discrimination. Hearing Research. 2006; 219(1-2):36-47. [DOI:10.1016/j.heares.2006.05.004] [PMID]
- Schow RL, Seikel JA, Chermak GD, Berent M. Central auditory processes and test measures: ASHA 1996 revisited. American Journal of Audiology. 2000; 9(2):63-8. [DOI:10.1044/1059-0889(2000/013)] [PMID]
- Domitz DM, Schow RL. A new CAPD battery--multiple auditory processing assessment: Factor analysis and comparisons with SCAN. American Journal of Audiology. 2000; 9(2):101-11. [DOI:10.1044/1059-0889(2000/012)] [PMID]
- American Academy of Audiology. American Academy of Audiology clinical practice guidelines: Diagnosis, treatment and management of children and adults with central auditory processing disorder. Fairfax: American Academy of Audiology; 2010. [Link]
- Khalfa S, Veuillet E, Collet L. Influence of handedness on peripheral auditory asymmetry. The European Journal of Neuroscience. 1998; 10(8):2731-7. [DOI:10.1046/j.1460-9568.1998.00286.x] [PMID]
- Lagacé J, Jutras B, Gagné JP. Auditory processing disorder and speech perception problems in noise: Finding the underlying origin. American Journal of Audiology. 2010; 19(1):17-25. [DOI:10.1044/1059-0889(2010/09-0022)] [PMID]
- McKeever WF, VanDeventer AD. Visual and auditory language processing asymmetries: Influences of handedeness, familial sinistrality, and sex. Cortex. 1977; 13(3):225-41. [DOI:10.1016/S0010-9452(77)80033-6] [PMID]
- Horbach M, Verhey JL, Hots J. On the pitch strength of bandpass noise in normal-hearing and hearing-impaired listeners. Trends in Hearing. 2018; 22:2331216518787067. [DOI:10.1177/2331216518787067] [PMID] [PMCID]
- McClaskey CM. Standard-interval size affects interval-discrimination thresholds for pure-tone melodic pitch intervals. Hearing Research. 2017; 355:64-69. [DOI:10.1016/j.heares.2017.09.008] [PMID] [PMCID]
- Nimmons GL, Kang RS, Drennan WR, Longnion J, Ruffin C, Worman T, et al. Clinical assessment of music perception in cochlear implant listeners. Otology & Neurotology. 2008; 29(2):149-55. [DOI:10.1097/mao.0b013e31812f7244] [PMID] [PMCID]
- Weisser S, Quanten M. Rethinking musical instrument classification: Towards a modular approach to the Hornbostel-Sachs system. Yearbook for Traditional Music. 2011; 43:122-45. [DOI:10.5921/yeartradmusi.43.0122]
- Mansouri P. [The basic theory of music (Persian)]. Tehran: Karnameh; 2017. [Link]
- Aarabi S, Jarollahi F, Jalaie S. Development and determination of the validity of Persian version of monaural selective auditory attention test in learning disabled children. Auditory and Vestibular Research. 2016.; 25(1):49-54. [Link]
- Tillery K. Central auditory processing evaluation: A test battery approach. In: Katz J, Medwetsky L, Burkard R, Hood L, editors. Handbook of clinical audiology. Baltimore: Lippincott Williams & Wilkins; 2009. [Link]
- Musiek FE. Assessment of central auditory dysfunction: the dichotic digit test revisited. Ear and Hearing. 1983; 4(2):79-83. [DOI:10.1097/00003446-198303000-00002] [PMID]
- Broadbent DE. The role of auditory localization in attention and memory span. Journal of Experimental Psychology. 1954; 47(3):191-6. [DOI:10.1037/h0054182] [PMID]
- Rajabpur E, Hajiablohasan F, Tahai SAA, Jalaie S. [Development of the Persian single dichotic digit test and its reliability in 7-9 year old male students (Persian)]. Bimonthly Audiology. 2014; 23(5):68-77. [Link]
- Rezapour M, Abdollahi FZ, Delphi M, Lotfi Y, Bakhshi EA. [Normalization and reliability evaluation of persian version of two-pair dichotic digits in 8 to 12-year-old children (Persian)]. Iranian Rehabilitation Journal. 2016; 14(2):115-20. [DOI:10.18869/nrip.irj.14.2.115]
- Pinheiro ML. Tests of central auditory function in children with learning disabilities. Central Auditory Dysfunction. 1977; 223-56. [Link]
- McDermott EE, Smart JL, Boiano JA, Bragg LE, Colon TN, Hanson EM, et al. Assessing auditory processing abilities in typically developing school-aged children. Journal of the American Academy of Audiology. 2016; 27(2):72-84. [DOI:10.3766/jaaa.14050] [PMID]
- Smart JL, Kuruvilla-Mathew A, Kelly AS, Purdy SC. Assessment of the efferent auditory system in children with suspected auditory processing disorder: The middle ear muscle reflex and contralateral inhibition of OAEs. International Journal of Audiology. 2019; 58(1):37-44. [DOI:10.1080/14992027.2018.1523578] [PMID]
- Musiek FE. Frequency (pitch) and duration pattern tests. Journal of the American Academy of Audiology. 1994; 5(4):265-8. [PMID]
- Musiek F, Pinheiro M. Frequency patterns in cochlear, brainstem, and cerebral lesions. Audiology. 1987; 26(2):79-88. [DOI:10.3109/00206098709078409]
- Shinn JB. Temporal processing: The basics. The Hearing Journal. 2003; 56(7):52. [DOI:10.1097/01.HJ.0000292557.52409.67]
- Alain C, Woods DL. Attention modulates auditory pattern memory as indexed by event-related brain potentials. Psychophysiology. 1997; 34(5):534-46. [DOI:10.1111/j.1469-8986.1997.tb01740.x] [PMID]
- Balen SA, Moore DR, Sameshima K. Pitch and duration pattern sequence tests in 7- to 11-year-old children: Results depend on response mode. Journal of the American Academy of Audiology. 2019; 30(1):6-15. [DOI:10.3766/jaaa.16132] [PMID] [PMCID]
- Musiek FE. The frequency pattern test: A guide. The Hearing Journal. 2002; 55(6):58-66. [DOI:10.1097/01.HJ.0000293280.99394.dd]
- Apfelstadt H. Effects of melodic perception instruction on pitch discrimination and vocal accuracy of kindergarten children. Journal of Research in Music Education. 1984; 32(1):15-24. [DOI:10.2307/3345277]
- Ahissar M. Dyslexia and the anchoring-deficit hypothesis. Trends in Cognitive Sciences. 2007; 11(11):458-65. [DOI:10.1016/j.tics.2007.08.015] [PMID]
- Harris JD. Discrimination of pitch; suggestions toward method and procedure. The American Journal of Psychology. 1948; 61(3):309-22. [DOI:10.2307/1417151] [PMID]
- Ahissar M, Lubin Y, Putter-Katz H, Banai K. Dyslexia and the failure to form a perceptual anchor. Nature Neuroscience. 2006; 9(12):1558-64. [DOI:10.1038/nn1800] [PMID]
- Best V, Ozmeral EJ, Kopco N, Shinn-Cunningham BG. Object continuity enhances selective auditory attention. Proc Natl Acad Sci USA. 2008; 105(35):13174-8. [DOI:10.1073/pnas.0803718105] [PMID] [PMCID]
- Sares AG, Foster NEV, Allen K, Hyde KL. Pitch and time processing in speech and tones: The effects of musical training and attention. Journal of Speech, Language, and Hearing Research. 2018; 61(3):496-509. [DOI:10.1044/2017_JSLHR-S-17-0207] [PMID]
Type of Study: Original |
Subject:
Audiometery
Received: 21/08/2023 | Accepted: 10/01/2024 | Published: 1/07/2024
Received: 21/08/2023 | Accepted: 10/01/2024 | Published: 1/07/2024
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
