

Volume 25, Issue 1 (Spring 2024)
jrehab 2024, 25(1): 134-157 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghadbeigi F, Alipour F, Ghaedamini Harouni G, Arabkari Z. Checking the Validity and Reliability of the Persian Version of the Resilience Assessment Questionnaire in Patients With Multiple Sclerosis. jrehab 2024; 25 (1) :134-157
URL: http://rehabilitationj.uswr.ac.ir/article-1-3282-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3282-en.html



1- Department of Social Work, School of Social Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Social Work, School of Social Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. , barbodalipour@gmail.com
3- Social Welfare Management Research Center, Social Health Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Social Work, School of Social Health, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. , barbodalipour@gmail.com
3- Social Welfare Management Research Center, Social Health Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 2525 kb]
(58 Downloads)
| Abstract (HTML) (413 Views)
Full-Text: (38 Views)
Introduction
Multiple sclerosis (MS) is a progressive and chronic immune-mediated neurological disease that primarily affects the spinal cord, brain, and optic nerves [1]. In MS, damage is done to the protective sheath of nerve fibers and causes inflammation. The exact cause of this disease is still unknown. Still, several possible causes are involved in this process, including weather conditions, autoimmune mechanisms, heredity, stress, immune deficiency, and environmental factors, especially viral infections. Common symptoms of this disease include fatigue, numbness, weakness of legs and arms, vision problems, imbalance, bladder and bowel dysfunction, sexual dysfunction, speech problems, depression and other emotional changes, movement, skill, communication, and activity limitations and difficulties [2].
The average age of onset of this disease is 20-30, and its prevalence is higher in women. MS is usually diagnosed in people aged 20-50 [3]. This disease is important because it affects people between the ages of 20 and 45, and this is when people enter the stage of continuing education, marriage, and work. This disease causes them significant disability [4]. This disease also causes a lot of worry and stress for patients and families, which can increase the severity of the disease [5].
In research conducted by Gromisch et al. entitled “using the resilience measuring tool of MS patients to identify psychological distress in MS People” in North America, the MS resiliency scale (MSRS) questionnaire was standardized [6] used In this study, by using the resilience measurement tool, the researcher tried to estimate the psychological distress of MS patients [6]took the help of 884 people with MS to conduct this research. The results have shown a strong negative correlation between resilience and mental distress in these people, so the lower the resilience score, the higher the possibility of mental distress in these people. According to the researchers, the resilience measurement tool has good validity and reliability for assessing different dimensions of resilience [7]. Nevertheless, there is still no tool available in Iran that has suitable psychometric properties to measure the resilience of MS patients for screening purposes and monitoring the impact of supportive interventions.
Among the tools that have been validated and made available to experts in the field of MS are things like the Persian version of the dynamic gait index test validated. Assesses the fatigue severity scale in MS patients. Therefore, this study was conducted to investigate the validity and reliability of the tool “measuring the resilience of MS patients” for use in the Iranian population and reporting its psychometric indicators.
Materials and Methods
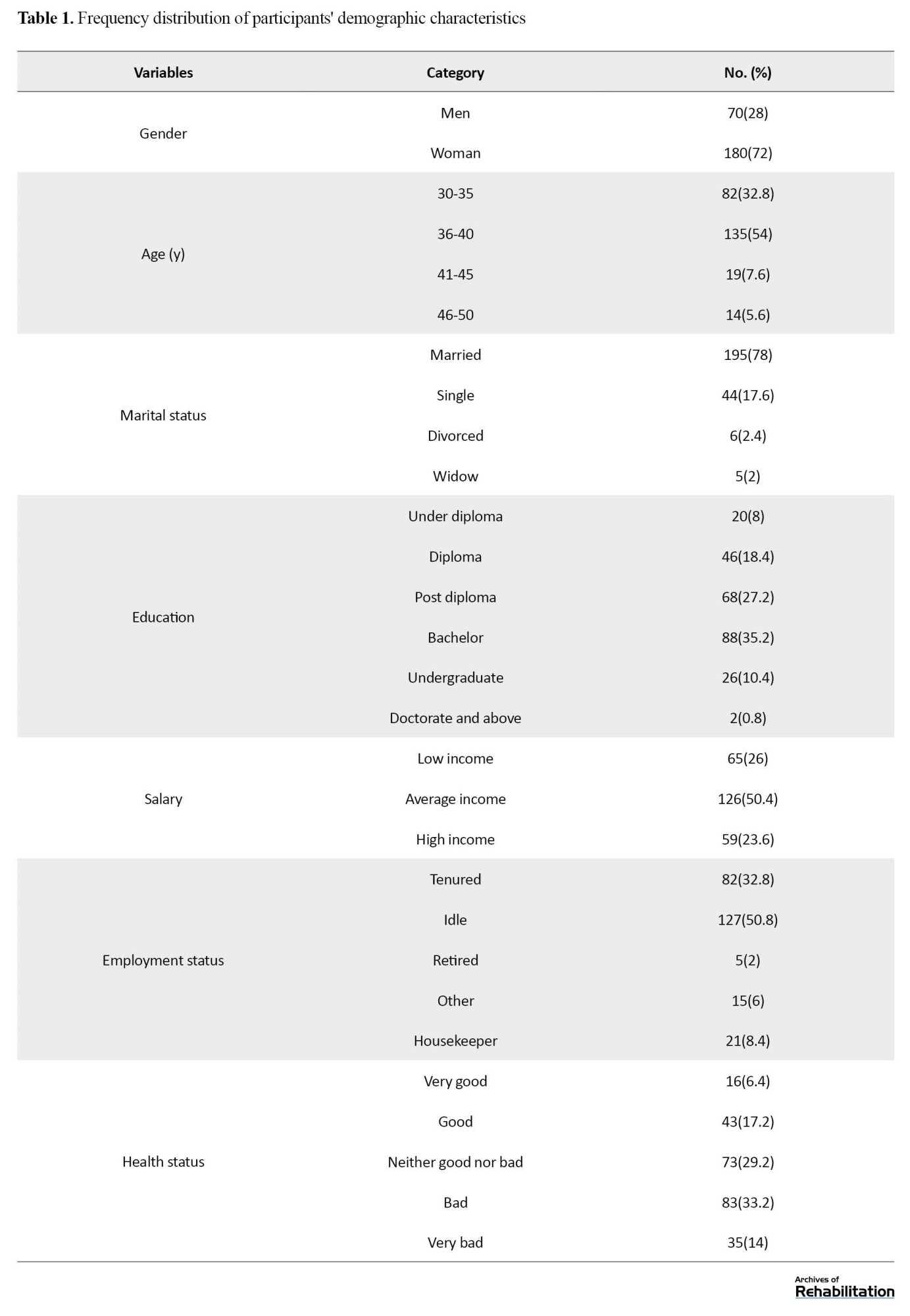
The method of the current research is descriptive and psychometric, and the statistical population of the current research includes all patients with MS living in Tehran City, Iran, in 2022. Of them, 250 patients who met the inclusion criteria were chosen by the available sampling. The criteria included having MS disease for a period of one year or more, having an age range of 18-60 years, agreeing to participate in a research based on signing a written consent form, being Iranian or fluent in the Persian language, being a member of MS Association centers, Hazrat Rasool Akram Hospital, Imam Hossein Hospital, and Rafidah Hospital, and filling out the research questionnaires. Due to the easy and simultaneous access to a large number of patients, the possibility of quick follow-up, and the cooperation of the heads of the centers, the mentioned hospitals entered the study cycle. The characteristics of participants are presented in Table 1.
Research tools
In this study, in addition to the resilience questionnaire, the hospital anxiety and depression questionnaire (HADS) was used. The reason for choosing this tool is its predictive validity, and this tool has also been used in the research of Gromisch et al. [6] to check its predictive validity. Below is the description of each questionnaire.
HADS was introduced and used for the first time by Zigmond and Snaith for screening psychiatric disorders in outpatient clinics of general hospitals [11]. This instrument measures depression and anxiety in outpatients. It is a 14-item self-report tool designed to screen the presence and occurrence of symptoms of anxiety and depression in patients during the last week. The duration of the implementation of this tool is less than 5 minutes, and the studied population ranges from teenagers aged 16 and above to older people. Sigmund and Sneath suggest that this scale be used for other groups. Each test component is scored on a scale of 0 to 3 [11]. Therefore, the scores of anxiety and depression subscales range from 0 to 21. For the two subscales, a score between 0 and 7 is considered normal, 8 to 10 mild, 11 to 14 moderate, and 15 to 21 severe. Using the Cronbach α coefficient, Kaviani et al. reported the internal consistency of this test as 0.70 for the depression subscale and 0.91 for the anxiety subscale, as well as the reliability coefficient using the open test method as 0.77 [12]. In this study, the Cronbach α was reported as 0.786 for anxiety symptoms and 0.791 for depression symptoms.
The MS resiliency scale (MSRS) questionnaire is a specific questionnaire used to measure the resilience of MS patients. Gromish and Zemon designed this uestionnaire in England in 2018. It includes 25 questions covering 5 areas: Physical activity and diet, peer support, family and friends support, spirituality, and emotional and cognitive strategies. The questions are scored on a 4-point Likert scale from “strongly agree” to “strongly disagree”, and the total score ranges from 0 to 100 [6]. Researchers use this self-report tool to measure the resilience of MS patients. In this tool, the scores are not “negative” or “positive” versus “false” or “true”. Still, higher scores in the questionnaire indicate a higher level of resilience, and lower scores indicate a lower level of resilience in this population. In addition, there is no specific number and value (cutoff point) regarding this scale’s ideal level of resilience. This tool has 5 subscales of emotional and cognitive strategies (10 items), physical activity and diet (6 items), peer support (2 items), family and friends support (5 items), and spirituality (2 items) [6]. This test has good construct validity, and its Cronbach α values for different subscales are between 0.929 and 0.799 [6]. The purpose of the present study is to investigate the psychometric properties of this tool among patients with MS.
Results
The first research findings are about whether the Persian version of the resilience questionnaire among patients with MS has adequate face validity.
For face validity, we tried to make the questionnaire understandable for the participants. To achieve this goal, the researcher asked 16 participants (due to the repeatability of the participants’ answers, face validity was done with 16 people) for whom this questionnaire was to be used. After obtaining their consent and explaining the study’s objectives, the questionnaire was given for review, and they were requested to comment on each item in the above cases. Then, 9 out of 20 items were modified and revised. The research’s second phase was implemented after modifying the questionnaire’s final form.
The second finding of the research is whether the Persian version of the resilience questionnaire among patients with MS has adequate content validity.
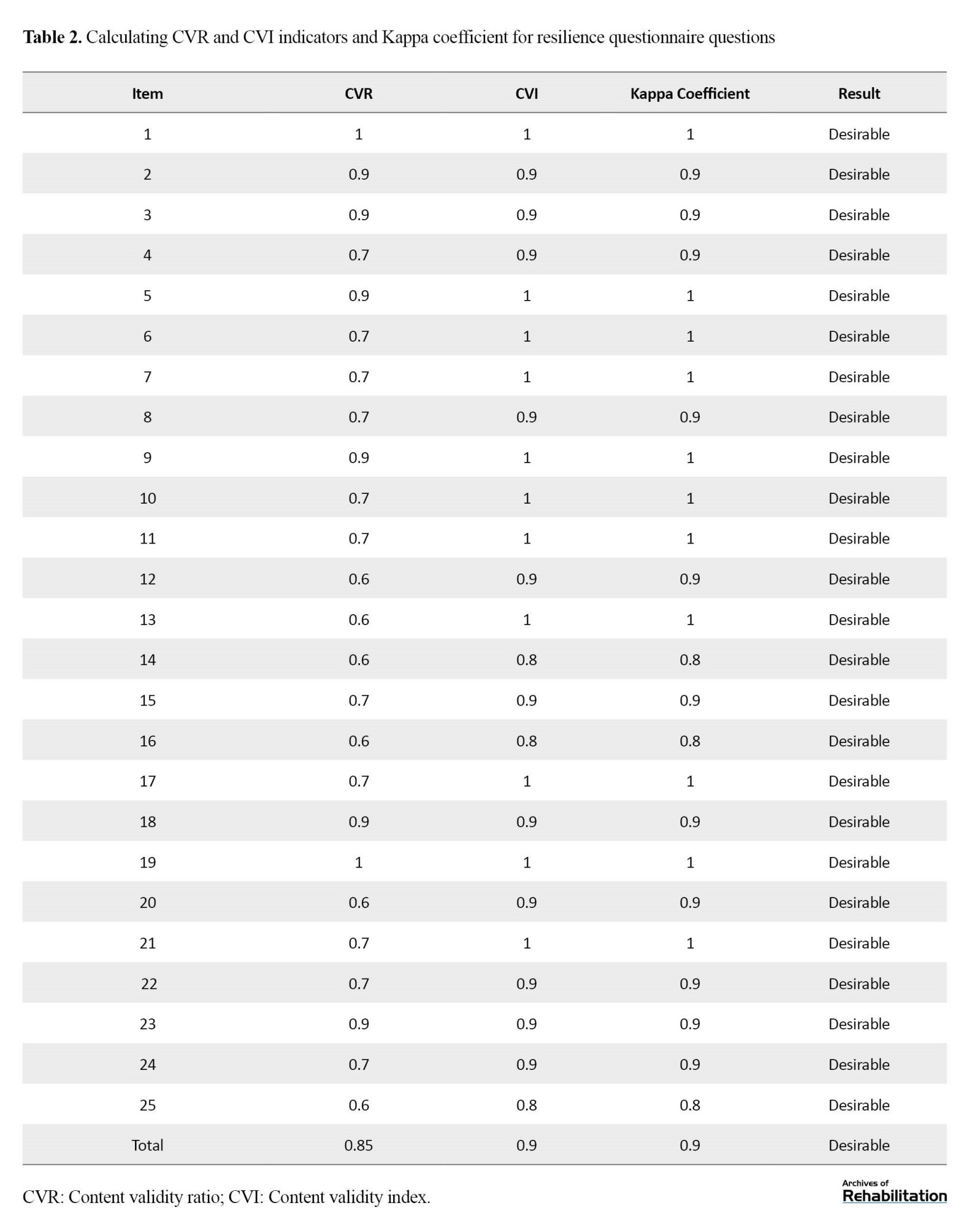
In the qualitative content validity phase of the MS patient resilience comparison questionnaire, the opinions of 20 experts in the field of research, tool-making psychologists, and counseling were sought. The proper place and appropriate scoring provided the necessary feedback, and then the questionnaire was modified according to the brief grammar suggestions. To determine quantitative content validity, the content validity ratio (CVR) and content validity index (CVI) of the questionnaire were calculated with the opinions of 20 counseling and psychology experts. The validity index of each questionnaire item was calculated, indicating the items’ appropriateness. Also, the result of the content validity index of the questions according to the calculated kappa was reported as favorable (Table 2).
The third finding of the research is whether the Persian version of the resilience questionnaire among patients with MS has adequate construct validity (factorial structure).
Exploratory factor analysis was used to check the construct validity. Exploratory factor analysis was done in stages. The factor structure of the 25-question resilience questionnaire was investigated by exploratory factor analysis. It should be noted that in the first stage, the structure of the questionnaire was examined by the method of factorization (principal components and axes) and two rotation methods (orthogonal/varimax and direct oblique/oblimin). The results indicated the sameness of both methods. For this reason, the factor analysis results are reported in the main axis method with varimax rotation. The assumptions of this test were checked to perform an exploratory factor analysis. Bartlett’s chi-square test determines the significance of the information in a matrix; the significance of this test is the minimum necessary condition to perform factor analysis. In Bartlett’s test, the null hypothesis is that the variables are only correlated with themselves, and the rejection of the null hypothesis indicates that the correlation matrix has significant information and that the minimum conditions necessary to perform factor analysis exist. In this study, the value of Bartlett’s sphericity test (χ2=2725, P=0.001) with a degree of freedom of 300 showed that this assumption is valid and the minimum condition for factor analysis is valid. In addition, the results revealed that the value of the sampling adequacy index of Keyser-Meyer-Elkin was equal to 0.84, and since the minimum value of this index to ensure the adequacy of the data matrix for operability is 0.70.The value obtained is higher than this value, so the factorial structure of the questionnaire was provided.
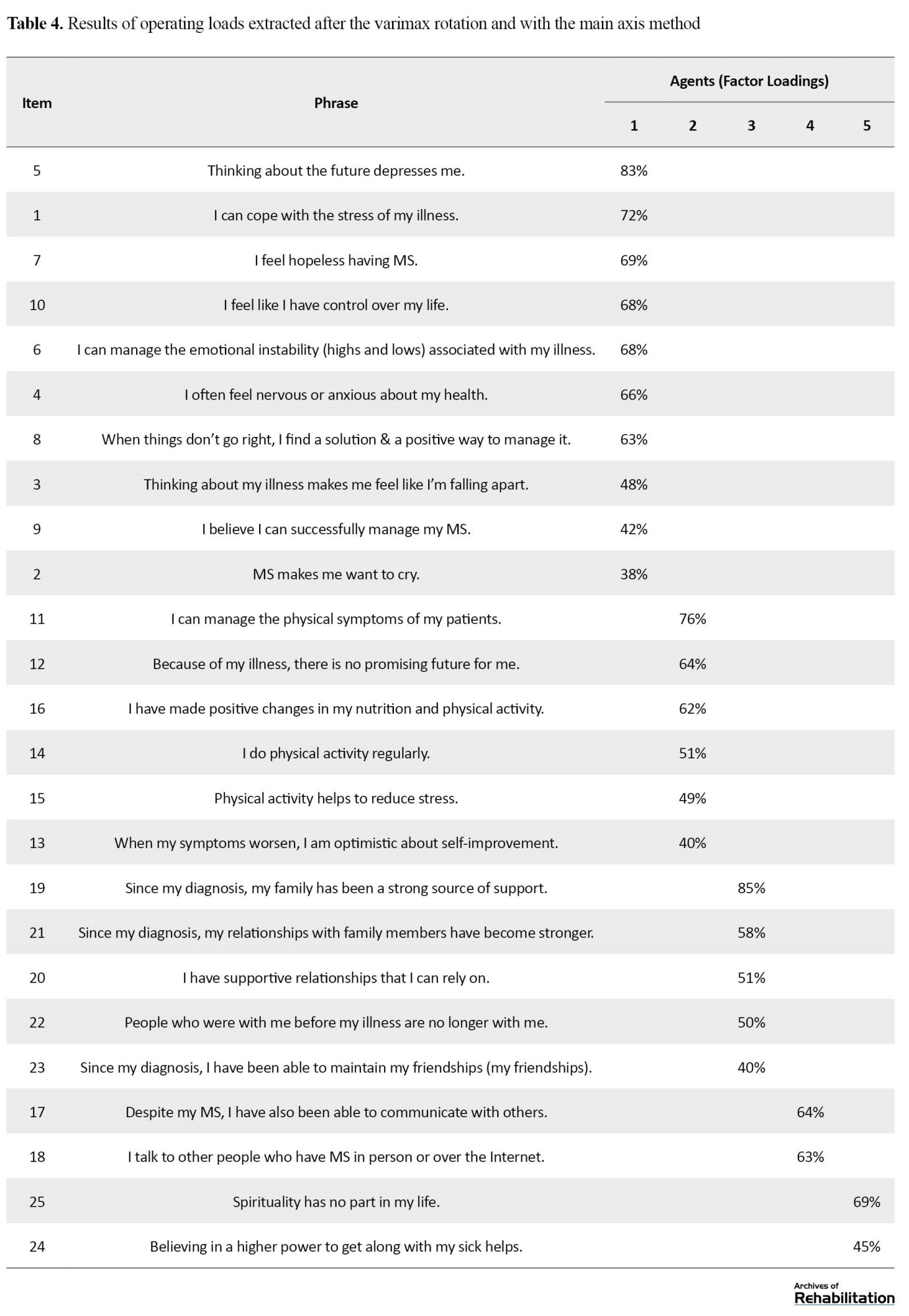
After investigating the indicators of sphericity and sampling adequacy, the factor structure of the questionnaire was checked with factor loadings higher than 0.40. The results showed that the structure of the questionnaire consists of 5 factors. The eigenvalues of the obtained factors were 6.86, 1.84, 1.22, 1.11, and 1, each of which was 27.45, 6.37, 4.88, and 4.44, respectively, and explained 3.84% of the variance and 47.96% of the variance in total. The factors extracted according to the questions loaded on each factor and the theoretical foundations include the research of Gromish et al. (2018) [5]. Emotional and cognitive strategies, physical activities and diet, friends and family support, peer support, and spirituality were named in order (Table 3).

Table 3 shows the factor loadings of each question on each factor. As described in the Table 3, the questions of the first factor are related to emotional and cognitive strategies. The results indicate that questions 1 to 10 have a factor loading only on the first factor. In factor analysis with the main axis, if an item has a load on two factors, it is interpreted according to its weight on one of them. In the first factor, the first question is interpreted on the first factor because it is part of the questions of the first factor. Question 15 has a similar situation. Therefore, according to the content of the question, it is interpreted as the second factor (Table 4).
To check the number of factors, attention was paid to things like eigenvalues higher than 1, the pebble diagram (Figure 1), the explained variance for each factor, and factor loadings higher than 0.32.
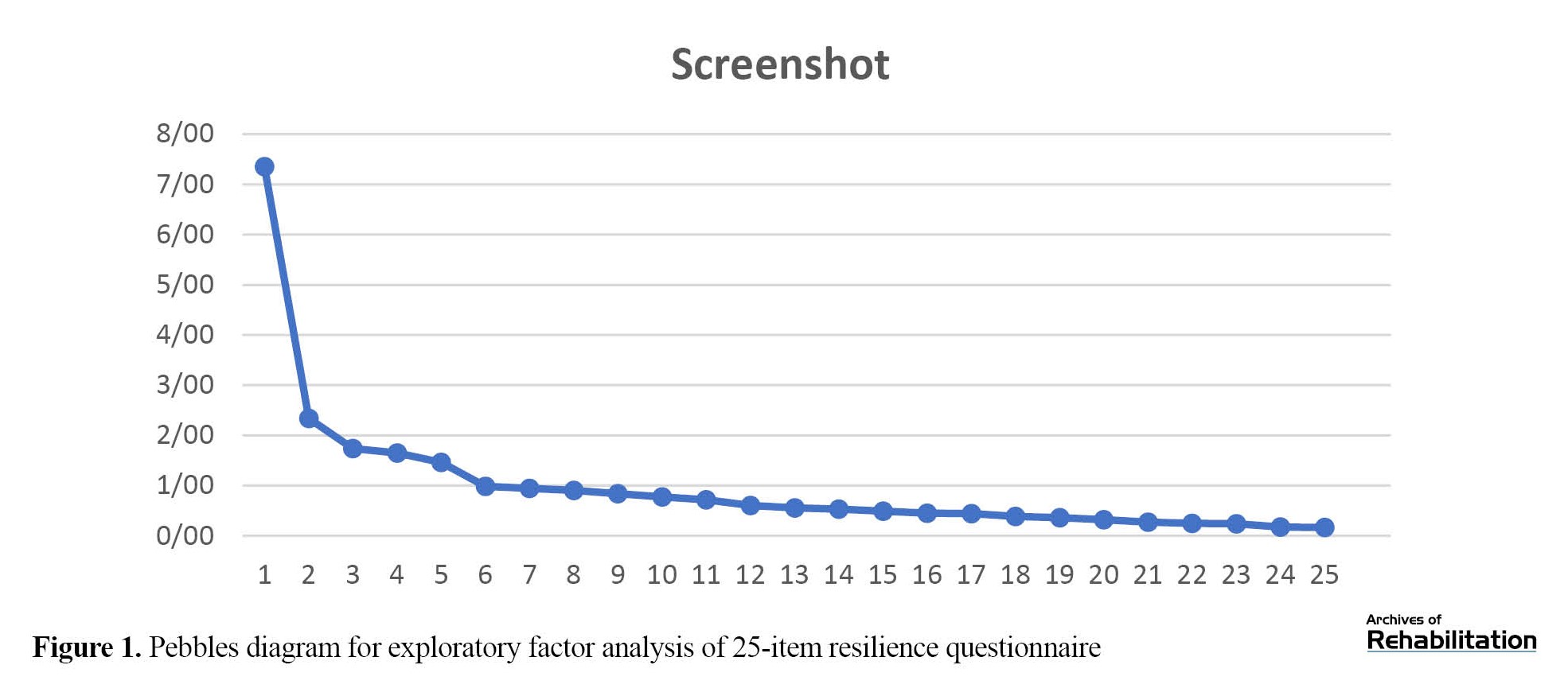 The eigenvalues reported in the Table of eigenvalues showed that no factor had an eigenvalue less than 1. In addition, these values are also presented in the gravel chart below. Also, according to the Table of factor loadings, the results indicate that no item has a factor loading less than 0.32. It should be noted that the value of 0.32 was chosen because at least one item must explain 10% of the variance, so if we increase 0.32 to the power, we will reach this value. Questions with factor loadings lower than this amount have no diagnostic value. Also, if the factor loading of each question is low, the variance explained for the factors is very small and cannot be considered a factor. According to the obtained results, it can be mentioned that the number of 5 factors is suitable.
The eigenvalues reported in the Table of eigenvalues showed that no factor had an eigenvalue less than 1. In addition, these values are also presented in the gravel chart below. Also, according to the Table of factor loadings, the results indicate that no item has a factor loading less than 0.32. It should be noted that the value of 0.32 was chosen because at least one item must explain 10% of the variance, so if we increase 0.32 to the power, we will reach this value. Questions with factor loadings lower than this amount have no diagnostic value. Also, if the factor loading of each question is low, the variance explained for the factors is very small and cannot be considered a factor. According to the obtained results, it can be mentioned that the number of 5 factors is suitable.
The fourth research question was whether the Persian version of the resilience questionnaire among patients with MS had adequate predictive validity.
To check the predictive validity of the resilience scale of MS patients, the HADS questionnaire was used, whose correlation matrix is reported in Table 5.
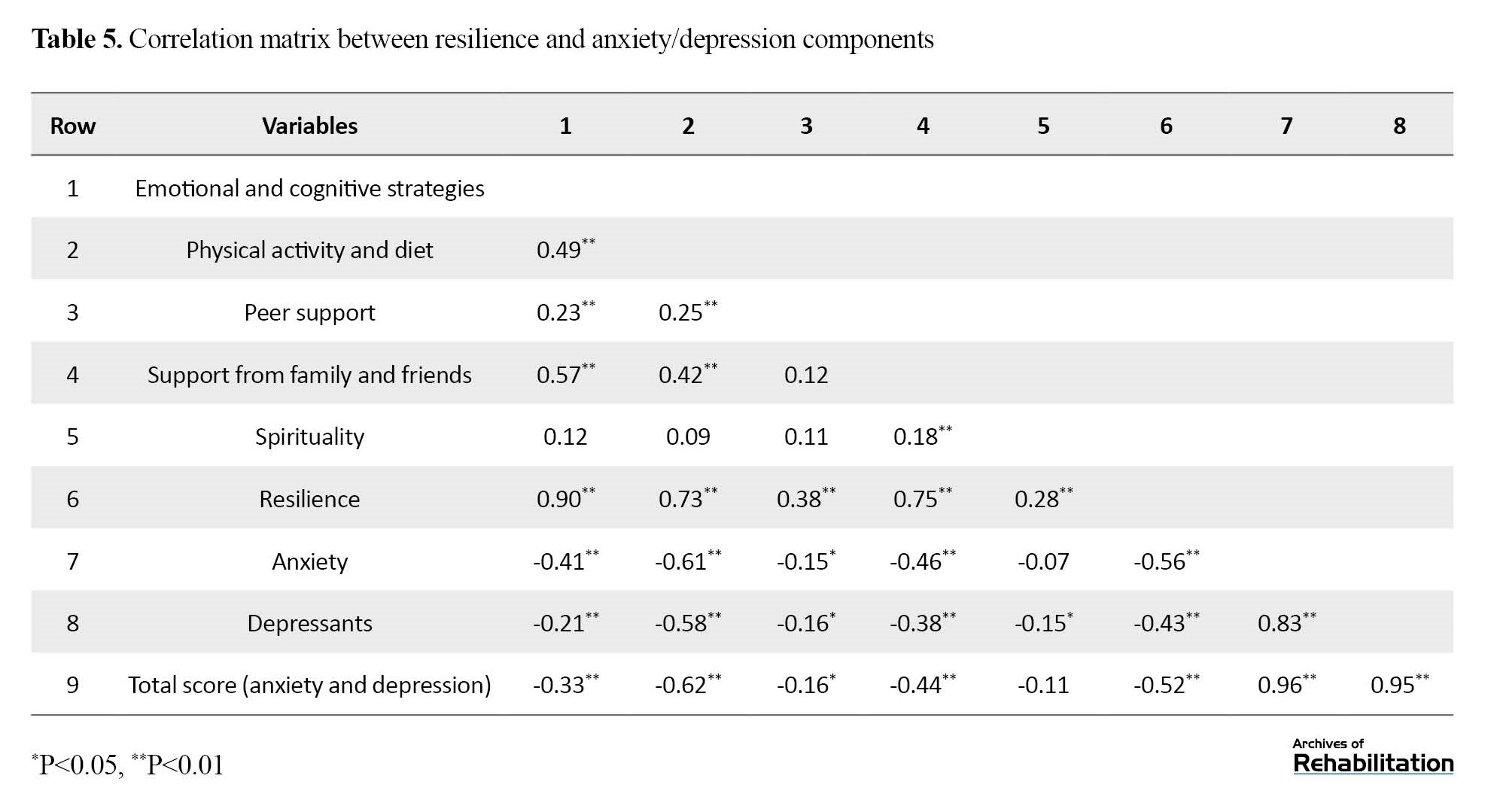
As seen in Table 5, the results showed that the components of “peer support” and “spirituality” have a lower correlation with anxiety and depression. Because the number of items of these two resilience components is probably very small. So, there are only two items for each component.
The fifth research question was whether the Persian version of the resilience questionnaire has adequate reliability among patients with MS.
The validity of the test was investigated using the Cronbach α and retest method. The Table 6 shows the Cronbach α of each resilience component and the entire questionnaire.
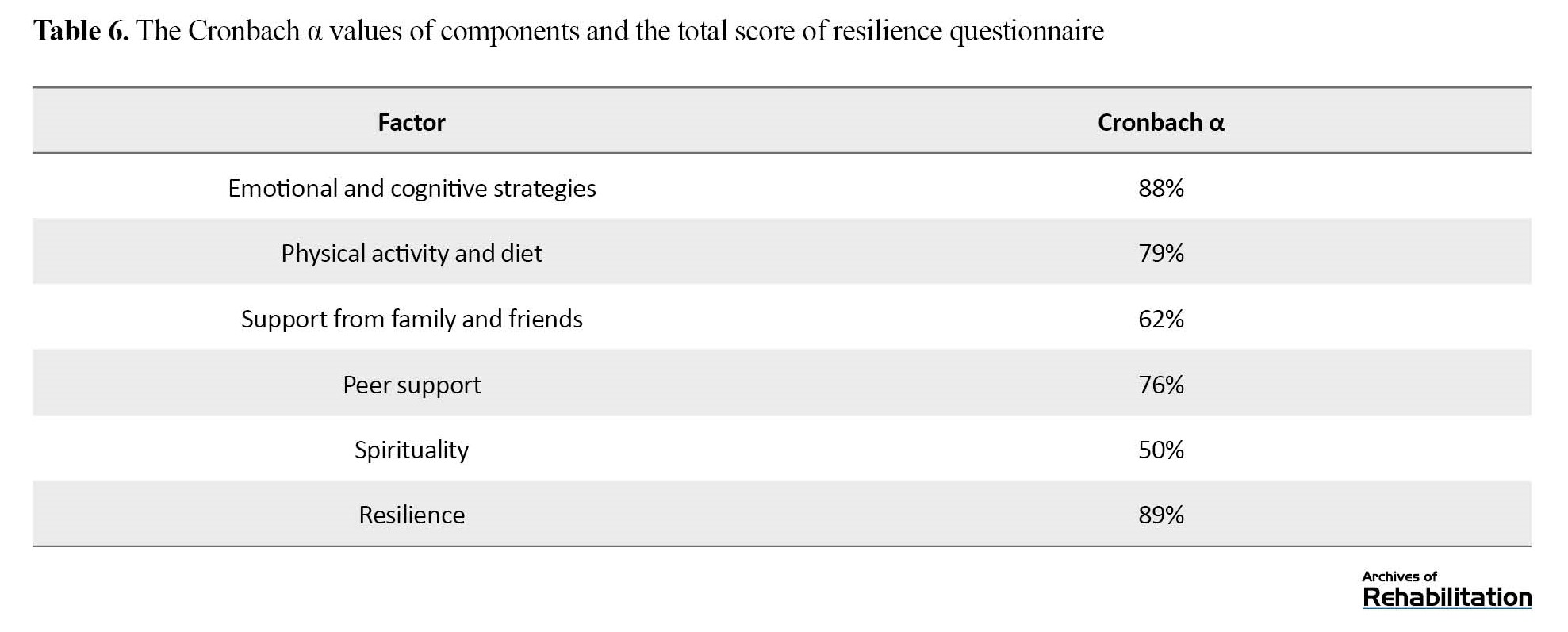
It should be noted that the α value is lower in components with a small number of items (family and peer support and spirituality).
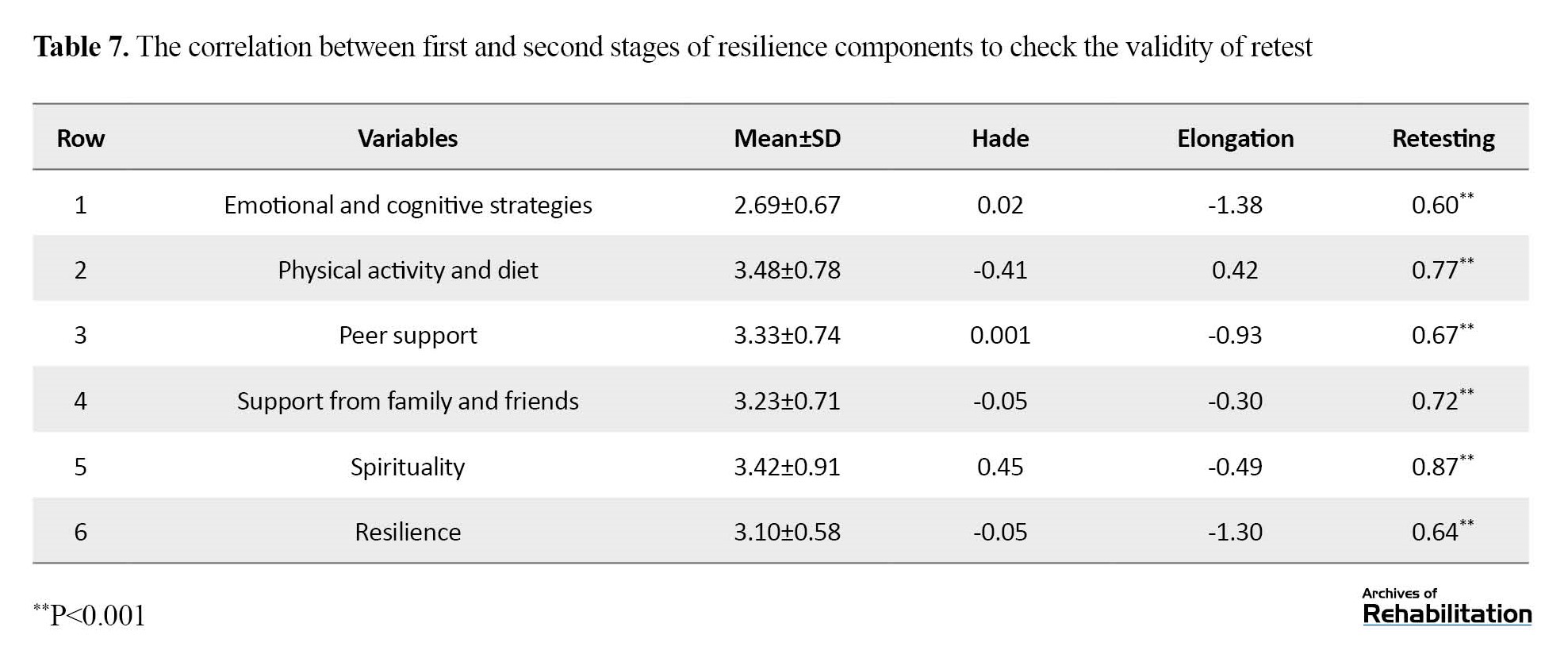
According to Table 6, the results of the Cronbach α to check the reliability of the test for the components of emotional and cognitive strategies, physical activity and diet, support of family and friends, support of peers, spirituality, and the total score of resilience are respectively 0.88. 0.79, 0.62, 0.76, 0.50, 0.89, showing the relatively favorable reliability of this tool. After checking the internal consistency using the Cronbach α method, the validity of the test was also calculated using the retest method. A total of 34 participants took part in the second phase after two months. The following Table shows the descriptive indices of resilience components in the second stage of measurement. In addition, the correlation between the first and second stages is shown as the calculation of retest validity in the last column of Table 7, showing that the validity of the test in the components and general is between 0.60 and 0.87.
Discussion
One of the important constructs of positive psychology is resilience, which emphasizes humans’ abilities and strong points. Resilience has an important role in mental health and in dealing with stressful conditions, including conditions of disease stress (like MS disease). Based on the results of the present study, the resilience scale can be used as a new tool to measure the resilience of MS patients with practical components that have valid and acceptable psychometric properties. Also, based on the results of this research, even though people with MS have higher resilience, they are somehow more exposed to anxiety and depression. Therefore, according to the results of this research and the importance of resilience among MS patients, the need to implement psychological interventions to improve these people’s resilience and psychological health should be stressed. In general, it can be concluded that the research is in line with the results of previous research by obtaining the desired reliability and validity, and this is a confirmation point that the resilience scale of MS patients can be used among this group.
This scale has good face validity, content validity, and internal consistency. Also, the results of this study confirmed the 5-factor nature of this scale, and all 5 subscales were also confirmed in Iranian culture. As a result, the diabetes annoyance scale with 25 items and 5 subscales of “emotional and cognitive strategies”, “physical activity and diet”, “support of friends”, “support of family and peers”, and “spirituality” was confirmed. This questionnaire can be used thanks to its simplicity, brevity, short-time execution, and self-reporting, especially in children. Also, this scale (resilience scale of MS patients) is the first Persian example of measuring the resilience of MS patients and is very useful for psychological, clinical, and research centers. Concerning aligning the current research findings with other research on the components found in the exploratory factor analysis, we can mention the following issues.
Emotional and cognitive strategies component
The name of this component agrees with the research of Gromisch et al. [6], Neto et al. [13], and Duan et al. [14]. The items of the first components of Gromisch et al.’s questionnaire [6] with the name of spirituality related to MS disease and the content of the items are similar to those of the components of “emotional and cognitive strategies” caused by MS disease in the present study. Negative problem orientation includes beliefs that express the perceived threat of problems, doubts about the ability to solve problems, and a tendency to be pessimistic about the outcome. A negative orientation to problem-solving is related to cognitions and emotions that hinder adaptive problem-solving and act as an obstacle in managing and reducing symptoms of psychological distress [15]. These thoughts are about lacking control over the disease (I feel in control of my life), hopelessness (I feel hopeless having MS), not having control over the disease (I can feel the emotional instabilities [highs and lows] associated with managing my illness), stress (I can cope with the stress of my illness), clutter (thinking about my illness makes me confused), depression (thinking about the future makes me depressed), and emotion dysregulation (I can manage emotional instabilities (highs and lows) related to my illness). Therefore, the results obtained from the present research align with the results of the mentioned research.
Physical activity and diet component
The naming of this component is consistent with the study of Gromisch et al.[6], Neto et al. [13], and Duan et al. [14]. The items of the first components of Gromisch et al.’s questionnaire [5] with the name of spirituality related to MS disease and the content of the items are similar to those of the components of emotional and cognitive strategies caused by MS disease in the present study. In the progress of this disease, a set of physical and mental problems arise. Accumulation of these problems affects most of a person’s daily activities, such as dressing, bathing, self-care, etc. [16]. Physical activity is an essential and influential resource in psychological, cognitive, and social health [6]. Therefore, regular participation in physical activity is necessary for health. People who actively participate in physical activities enjoy a higher level of physical fitness and are at lower risk of many debilitating medical conditions than inactive people. It is widely recognized that the health benefits of participating in physical activities include physical and mental health [17]. Liśkiewicz et al. [18] reported that physical activity is associated with many functional, cellular, and molecular changes in the brain, improves mood and cognition, and accelerates hippocampus neurogenesis. This issue can enhance resilience in a person. Also, various research has shown that lifestyle (such as physical activities, diet, etc.) can significantly improve people’s resilience. Therefore, the results obtained from the present research align with the results of the mentioned research.
Family and friends support, peer support component
This component’s naming is consistent with Gromisch et al. [6], Neto et al. [13], and Duan et al. [14]. The items of the third and fourth components of the questionnaire of Gromisch et al. [6] with the names of peer support, family, and friend support related to MS, and the content of the items are also similar to the items of the components of peer support and family support and friend support caused by the MS disease in the present study. Social support is the strongest coping force for a person to face successfully and easily when dealing with stressful situations. It facilitates the tolerance of problems for patients [18]. Support from family, friends, and important peers plays an important and prominent role in strengthening and expanding individual resilience in society [19]. Social support is the help that a person receives from family, friends, and peers in stressful situations and is known as one of the most powerful coping forces for successful and easy coping of people in high-risk and stressful situations [14]. Bernard [20]considered supportive and caring relationships an essential source of resilience. He stated that the people who provide this type of support are influential people who provide intimacy, care, and attention while helping the individual. They do so that he knows his capabilities and resources better. From his point of view, one aspect of the social environment that promotes resilience is providing opportunities for participation and cooperation. Also, its sensitivity in a group is a stable feeling of two-way interaction in a special period [20]. Therefore, in general, social support (family, friends, and peers) can affect resilience in MS patients, which means that the presence of social support strengthens and increases resilience, and the absence of social support can cause low resilience in MS patients. The results of the present study are consistent with the results of Benard [20] and Hajmohammadi and Shirazi [7].
Spirituality component
The naming of this component is consistent with the research of Gromisch et al. [5], Neto et al. [12], and Doan et al. [14]. The items of the fifth component of Gromis et al.’s questionnaire [6] with the name of spirituality related to MS disease and the content of the items are also similar to the items of spirituality components caused by MS disease in the present study. Many researchers have shown the positive effect of spirituality and religious factors in increasing the level of wellbeing and mental health, improving mental and physical diseases, making people resistant to tension, anxiety, and depression, and creating hope, peace, meaningfulness, and happiness. Some psychological research has been conducted on the effect of spirituality and religious beliefs on the adaptation of people with different conditions, including disease. Current theories in spirituality and religious beliefs support the idea that spirituality and religious beliefs are complex phenomena and have various effects on health, adaptation of people to new conditions (including illness), and resilience [21]. Hajmohammadi and Shirazi [7] believed that spirituality reduces mental disturbances, improves coping strategies and quality of life, and improves resilience in people. Therefore, the existence of spirituality in people makes them more resilient. Various studies have shown that spirituality makes people more resilient against MS [21]. Hence, the results obtained from the present research align with the results of the mentioned research.
Conclusion
Based on the results obtained from this research, i.e. the acceptable validity and reliability of the studied tool, researchers interested in examining the resilience variable can benefit from this scale to achieve their research goals.
Some limitations of the current research are as follows. Because the sample of this research was selected as available, caution should be taken in generalizing its results to other societies. The degree of cooperation of the interviewees and the respondents to the questionnaires and their honesty in answering the questions are among the things that are almost out of the researcher’s will and control and can affect the research results.
Research proposals
Due to the novelty of this issue, researchers can use the theoretical foundations of this research as criteria and propose and test several hypotheses based on it. This research can be the source of other research and help to develop knowledge in this field. In future research, the statistical population of MS patients can be used, and other patients can be used. It is suggested that this research be conducted again on a random sample to make its results more generalizable. It is proposed to utilize the resilience questionnaire of MS patients, whose validity and reliability were examined and confirmed in this study, for clinical screening, evaluation, and research. Due to the impact of resilience on the health of patients with MS, it is recommended to use resilience intervention programs for patients with MS.
Ethical Considerations
Compliance with ethical guidelines
At the beginning of the interview, the purpose of the study, and data confidentiality were explained to the participants and written and verbal consent were obtained. The subjects had the right to withdraw from the study at any time. The study has been approved by research committee of University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1401.083)
Funding
The present article was extracted from the master's thesis of Fatemeh Qadbigi, approved by Department of Social Work, School of Social Health, University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Conceptualization: Fardin Alipour; Design of study: Fatemeh Ghadbeigi and Fardin Alipour; Data collection: Fatemeh Ghadbeigi; Data analysis: Fatemeh Ghadbeigi and Gholamreza Ghaedamini Harouni; Formal analysis: Fardin Alipour; Revising the manuscript: Fardin Alipour and Zoleikha Arabkari; Reading and approving the final manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
Reference
Multiple sclerosis (MS) is a progressive and chronic immune-mediated neurological disease that primarily affects the spinal cord, brain, and optic nerves [1]. In MS, damage is done to the protective sheath of nerve fibers and causes inflammation. The exact cause of this disease is still unknown. Still, several possible causes are involved in this process, including weather conditions, autoimmune mechanisms, heredity, stress, immune deficiency, and environmental factors, especially viral infections. Common symptoms of this disease include fatigue, numbness, weakness of legs and arms, vision problems, imbalance, bladder and bowel dysfunction, sexual dysfunction, speech problems, depression and other emotional changes, movement, skill, communication, and activity limitations and difficulties [2].
The average age of onset of this disease is 20-30, and its prevalence is higher in women. MS is usually diagnosed in people aged 20-50 [3]. This disease is important because it affects people between the ages of 20 and 45, and this is when people enter the stage of continuing education, marriage, and work. This disease causes them significant disability [4]. This disease also causes a lot of worry and stress for patients and families, which can increase the severity of the disease [5].
In research conducted by Gromisch et al. entitled “using the resilience measuring tool of MS patients to identify psychological distress in MS People” in North America, the MS resiliency scale (MSRS) questionnaire was standardized [6] used In this study, by using the resilience measurement tool, the researcher tried to estimate the psychological distress of MS patients [6]took the help of 884 people with MS to conduct this research. The results have shown a strong negative correlation between resilience and mental distress in these people, so the lower the resilience score, the higher the possibility of mental distress in these people. According to the researchers, the resilience measurement tool has good validity and reliability for assessing different dimensions of resilience [7]. Nevertheless, there is still no tool available in Iran that has suitable psychometric properties to measure the resilience of MS patients for screening purposes and monitoring the impact of supportive interventions.
Among the tools that have been validated and made available to experts in the field of MS are things like the Persian version of the dynamic gait index test validated. Assesses the fatigue severity scale in MS patients. Therefore, this study was conducted to investigate the validity and reliability of the tool “measuring the resilience of MS patients” for use in the Iranian population and reporting its psychometric indicators.
Materials and Methods
The method of the current research is descriptive and psychometric, and the statistical population of the current research includes all patients with MS living in Tehran City, Iran, in 2022. Of them, 250 patients who met the inclusion criteria were chosen by the available sampling. The criteria included having MS disease for a period of one year or more, having an age range of 18-60 years, agreeing to participate in a research based on signing a written consent form, being Iranian or fluent in the Persian language, being a member of MS Association centers, Hazrat Rasool Akram Hospital, Imam Hossein Hospital, and Rafidah Hospital, and filling out the research questionnaires. Due to the easy and simultaneous access to a large number of patients, the possibility of quick follow-up, and the cooperation of the heads of the centers, the mentioned hospitals entered the study cycle. The characteristics of participants are presented in Table 1.
Research tools
In this study, in addition to the resilience questionnaire, the hospital anxiety and depression questionnaire (HADS) was used. The reason for choosing this tool is its predictive validity, and this tool has also been used in the research of Gromisch et al. [6] to check its predictive validity. Below is the description of each questionnaire.
HADS was introduced and used for the first time by Zigmond and Snaith for screening psychiatric disorders in outpatient clinics of general hospitals [11]. This instrument measures depression and anxiety in outpatients. It is a 14-item self-report tool designed to screen the presence and occurrence of symptoms of anxiety and depression in patients during the last week. The duration of the implementation of this tool is less than 5 minutes, and the studied population ranges from teenagers aged 16 and above to older people. Sigmund and Sneath suggest that this scale be used for other groups. Each test component is scored on a scale of 0 to 3 [11]. Therefore, the scores of anxiety and depression subscales range from 0 to 21. For the two subscales, a score between 0 and 7 is considered normal, 8 to 10 mild, 11 to 14 moderate, and 15 to 21 severe. Using the Cronbach α coefficient, Kaviani et al. reported the internal consistency of this test as 0.70 for the depression subscale and 0.91 for the anxiety subscale, as well as the reliability coefficient using the open test method as 0.77 [12]. In this study, the Cronbach α was reported as 0.786 for anxiety symptoms and 0.791 for depression symptoms.
The MS resiliency scale (MSRS) questionnaire is a specific questionnaire used to measure the resilience of MS patients. Gromish and Zemon designed this uestionnaire in England in 2018. It includes 25 questions covering 5 areas: Physical activity and diet, peer support, family and friends support, spirituality, and emotional and cognitive strategies. The questions are scored on a 4-point Likert scale from “strongly agree” to “strongly disagree”, and the total score ranges from 0 to 100 [6]. Researchers use this self-report tool to measure the resilience of MS patients. In this tool, the scores are not “negative” or “positive” versus “false” or “true”. Still, higher scores in the questionnaire indicate a higher level of resilience, and lower scores indicate a lower level of resilience in this population. In addition, there is no specific number and value (cutoff point) regarding this scale’s ideal level of resilience. This tool has 5 subscales of emotional and cognitive strategies (10 items), physical activity and diet (6 items), peer support (2 items), family and friends support (5 items), and spirituality (2 items) [6]. This test has good construct validity, and its Cronbach α values for different subscales are between 0.929 and 0.799 [6]. The purpose of the present study is to investigate the psychometric properties of this tool among patients with MS.
Results
The first research findings are about whether the Persian version of the resilience questionnaire among patients with MS has adequate face validity.
For face validity, we tried to make the questionnaire understandable for the participants. To achieve this goal, the researcher asked 16 participants (due to the repeatability of the participants’ answers, face validity was done with 16 people) for whom this questionnaire was to be used. After obtaining their consent and explaining the study’s objectives, the questionnaire was given for review, and they were requested to comment on each item in the above cases. Then, 9 out of 20 items were modified and revised. The research’s second phase was implemented after modifying the questionnaire’s final form.
The second finding of the research is whether the Persian version of the resilience questionnaire among patients with MS has adequate content validity.
In the qualitative content validity phase of the MS patient resilience comparison questionnaire, the opinions of 20 experts in the field of research, tool-making psychologists, and counseling were sought. The proper place and appropriate scoring provided the necessary feedback, and then the questionnaire was modified according to the brief grammar suggestions. To determine quantitative content validity, the content validity ratio (CVR) and content validity index (CVI) of the questionnaire were calculated with the opinions of 20 counseling and psychology experts. The validity index of each questionnaire item was calculated, indicating the items’ appropriateness. Also, the result of the content validity index of the questions according to the calculated kappa was reported as favorable (Table 2).
The third finding of the research is whether the Persian version of the resilience questionnaire among patients with MS has adequate construct validity (factorial structure).
Exploratory factor analysis was used to check the construct validity. Exploratory factor analysis was done in stages. The factor structure of the 25-question resilience questionnaire was investigated by exploratory factor analysis. It should be noted that in the first stage, the structure of the questionnaire was examined by the method of factorization (principal components and axes) and two rotation methods (orthogonal/varimax and direct oblique/oblimin). The results indicated the sameness of both methods. For this reason, the factor analysis results are reported in the main axis method with varimax rotation. The assumptions of this test were checked to perform an exploratory factor analysis. Bartlett’s chi-square test determines the significance of the information in a matrix; the significance of this test is the minimum necessary condition to perform factor analysis. In Bartlett’s test, the null hypothesis is that the variables are only correlated with themselves, and the rejection of the null hypothesis indicates that the correlation matrix has significant information and that the minimum conditions necessary to perform factor analysis exist. In this study, the value of Bartlett’s sphericity test (χ2=2725, P=0.001) with a degree of freedom of 300 showed that this assumption is valid and the minimum condition for factor analysis is valid. In addition, the results revealed that the value of the sampling adequacy index of Keyser-Meyer-Elkin was equal to 0.84, and since the minimum value of this index to ensure the adequacy of the data matrix for operability is 0.70.The value obtained is higher than this value, so the factorial structure of the questionnaire was provided.
After investigating the indicators of sphericity and sampling adequacy, the factor structure of the questionnaire was checked with factor loadings higher than 0.40. The results showed that the structure of the questionnaire consists of 5 factors. The eigenvalues of the obtained factors were 6.86, 1.84, 1.22, 1.11, and 1, each of which was 27.45, 6.37, 4.88, and 4.44, respectively, and explained 3.84% of the variance and 47.96% of the variance in total. The factors extracted according to the questions loaded on each factor and the theoretical foundations include the research of Gromish et al. (2018) [5]. Emotional and cognitive strategies, physical activities and diet, friends and family support, peer support, and spirituality were named in order (Table 3).
Table 3 shows the factor loadings of each question on each factor. As described in the Table 3, the questions of the first factor are related to emotional and cognitive strategies. The results indicate that questions 1 to 10 have a factor loading only on the first factor. In factor analysis with the main axis, if an item has a load on two factors, it is interpreted according to its weight on one of them. In the first factor, the first question is interpreted on the first factor because it is part of the questions of the first factor. Question 15 has a similar situation. Therefore, according to the content of the question, it is interpreted as the second factor (Table 4).
To check the number of factors, attention was paid to things like eigenvalues higher than 1, the pebble diagram (Figure 1), the explained variance for each factor, and factor loadings higher than 0.32.
The fourth research question was whether the Persian version of the resilience questionnaire among patients with MS had adequate predictive validity.
To check the predictive validity of the resilience scale of MS patients, the HADS questionnaire was used, whose correlation matrix is reported in Table 5.
As seen in Table 5, the results showed that the components of “peer support” and “spirituality” have a lower correlation with anxiety and depression. Because the number of items of these two resilience components is probably very small. So, there are only two items for each component.
The fifth research question was whether the Persian version of the resilience questionnaire has adequate reliability among patients with MS.
The validity of the test was investigated using the Cronbach α and retest method. The Table 6 shows the Cronbach α of each resilience component and the entire questionnaire.
It should be noted that the α value is lower in components with a small number of items (family and peer support and spirituality).
According to Table 6, the results of the Cronbach α to check the reliability of the test for the components of emotional and cognitive strategies, physical activity and diet, support of family and friends, support of peers, spirituality, and the total score of resilience are respectively 0.88. 0.79, 0.62, 0.76, 0.50, 0.89, showing the relatively favorable reliability of this tool. After checking the internal consistency using the Cronbach α method, the validity of the test was also calculated using the retest method. A total of 34 participants took part in the second phase after two months. The following Table shows the descriptive indices of resilience components in the second stage of measurement. In addition, the correlation between the first and second stages is shown as the calculation of retest validity in the last column of Table 7, showing that the validity of the test in the components and general is between 0.60 and 0.87.
Discussion
One of the important constructs of positive psychology is resilience, which emphasizes humans’ abilities and strong points. Resilience has an important role in mental health and in dealing with stressful conditions, including conditions of disease stress (like MS disease). Based on the results of the present study, the resilience scale can be used as a new tool to measure the resilience of MS patients with practical components that have valid and acceptable psychometric properties. Also, based on the results of this research, even though people with MS have higher resilience, they are somehow more exposed to anxiety and depression. Therefore, according to the results of this research and the importance of resilience among MS patients, the need to implement psychological interventions to improve these people’s resilience and psychological health should be stressed. In general, it can be concluded that the research is in line with the results of previous research by obtaining the desired reliability and validity, and this is a confirmation point that the resilience scale of MS patients can be used among this group.
This scale has good face validity, content validity, and internal consistency. Also, the results of this study confirmed the 5-factor nature of this scale, and all 5 subscales were also confirmed in Iranian culture. As a result, the diabetes annoyance scale with 25 items and 5 subscales of “emotional and cognitive strategies”, “physical activity and diet”, “support of friends”, “support of family and peers”, and “spirituality” was confirmed. This questionnaire can be used thanks to its simplicity, brevity, short-time execution, and self-reporting, especially in children. Also, this scale (resilience scale of MS patients) is the first Persian example of measuring the resilience of MS patients and is very useful for psychological, clinical, and research centers. Concerning aligning the current research findings with other research on the components found in the exploratory factor analysis, we can mention the following issues.
Emotional and cognitive strategies component
The name of this component agrees with the research of Gromisch et al. [6], Neto et al. [13], and Duan et al. [14]. The items of the first components of Gromisch et al.’s questionnaire [6] with the name of spirituality related to MS disease and the content of the items are similar to those of the components of “emotional and cognitive strategies” caused by MS disease in the present study. Negative problem orientation includes beliefs that express the perceived threat of problems, doubts about the ability to solve problems, and a tendency to be pessimistic about the outcome. A negative orientation to problem-solving is related to cognitions and emotions that hinder adaptive problem-solving and act as an obstacle in managing and reducing symptoms of psychological distress [15]. These thoughts are about lacking control over the disease (I feel in control of my life), hopelessness (I feel hopeless having MS), not having control over the disease (I can feel the emotional instabilities [highs and lows] associated with managing my illness), stress (I can cope with the stress of my illness), clutter (thinking about my illness makes me confused), depression (thinking about the future makes me depressed), and emotion dysregulation (I can manage emotional instabilities (highs and lows) related to my illness). Therefore, the results obtained from the present research align with the results of the mentioned research.
Physical activity and diet component
The naming of this component is consistent with the study of Gromisch et al.[6], Neto et al. [13], and Duan et al. [14]. The items of the first components of Gromisch et al.’s questionnaire [5] with the name of spirituality related to MS disease and the content of the items are similar to those of the components of emotional and cognitive strategies caused by MS disease in the present study. In the progress of this disease, a set of physical and mental problems arise. Accumulation of these problems affects most of a person’s daily activities, such as dressing, bathing, self-care, etc. [16]. Physical activity is an essential and influential resource in psychological, cognitive, and social health [6]. Therefore, regular participation in physical activity is necessary for health. People who actively participate in physical activities enjoy a higher level of physical fitness and are at lower risk of many debilitating medical conditions than inactive people. It is widely recognized that the health benefits of participating in physical activities include physical and mental health [17]. Liśkiewicz et al. [18] reported that physical activity is associated with many functional, cellular, and molecular changes in the brain, improves mood and cognition, and accelerates hippocampus neurogenesis. This issue can enhance resilience in a person. Also, various research has shown that lifestyle (such as physical activities, diet, etc.) can significantly improve people’s resilience. Therefore, the results obtained from the present research align with the results of the mentioned research.
Family and friends support, peer support component
This component’s naming is consistent with Gromisch et al. [6], Neto et al. [13], and Duan et al. [14]. The items of the third and fourth components of the questionnaire of Gromisch et al. [6] with the names of peer support, family, and friend support related to MS, and the content of the items are also similar to the items of the components of peer support and family support and friend support caused by the MS disease in the present study. Social support is the strongest coping force for a person to face successfully and easily when dealing with stressful situations. It facilitates the tolerance of problems for patients [18]. Support from family, friends, and important peers plays an important and prominent role in strengthening and expanding individual resilience in society [19]. Social support is the help that a person receives from family, friends, and peers in stressful situations and is known as one of the most powerful coping forces for successful and easy coping of people in high-risk and stressful situations [14]. Bernard [20]considered supportive and caring relationships an essential source of resilience. He stated that the people who provide this type of support are influential people who provide intimacy, care, and attention while helping the individual. They do so that he knows his capabilities and resources better. From his point of view, one aspect of the social environment that promotes resilience is providing opportunities for participation and cooperation. Also, its sensitivity in a group is a stable feeling of two-way interaction in a special period [20]. Therefore, in general, social support (family, friends, and peers) can affect resilience in MS patients, which means that the presence of social support strengthens and increases resilience, and the absence of social support can cause low resilience in MS patients. The results of the present study are consistent with the results of Benard [20] and Hajmohammadi and Shirazi [7].
Spirituality component
The naming of this component is consistent with the research of Gromisch et al. [5], Neto et al. [12], and Doan et al. [14]. The items of the fifth component of Gromis et al.’s questionnaire [6] with the name of spirituality related to MS disease and the content of the items are also similar to the items of spirituality components caused by MS disease in the present study. Many researchers have shown the positive effect of spirituality and religious factors in increasing the level of wellbeing and mental health, improving mental and physical diseases, making people resistant to tension, anxiety, and depression, and creating hope, peace, meaningfulness, and happiness. Some psychological research has been conducted on the effect of spirituality and religious beliefs on the adaptation of people with different conditions, including disease. Current theories in spirituality and religious beliefs support the idea that spirituality and religious beliefs are complex phenomena and have various effects on health, adaptation of people to new conditions (including illness), and resilience [21]. Hajmohammadi and Shirazi [7] believed that spirituality reduces mental disturbances, improves coping strategies and quality of life, and improves resilience in people. Therefore, the existence of spirituality in people makes them more resilient. Various studies have shown that spirituality makes people more resilient against MS [21]. Hence, the results obtained from the present research align with the results of the mentioned research.
Conclusion
Based on the results obtained from this research, i.e. the acceptable validity and reliability of the studied tool, researchers interested in examining the resilience variable can benefit from this scale to achieve their research goals.
Some limitations of the current research are as follows. Because the sample of this research was selected as available, caution should be taken in generalizing its results to other societies. The degree of cooperation of the interviewees and the respondents to the questionnaires and their honesty in answering the questions are among the things that are almost out of the researcher’s will and control and can affect the research results.
Research proposals
Due to the novelty of this issue, researchers can use the theoretical foundations of this research as criteria and propose and test several hypotheses based on it. This research can be the source of other research and help to develop knowledge in this field. In future research, the statistical population of MS patients can be used, and other patients can be used. It is suggested that this research be conducted again on a random sample to make its results more generalizable. It is proposed to utilize the resilience questionnaire of MS patients, whose validity and reliability were examined and confirmed in this study, for clinical screening, evaluation, and research. Due to the impact of resilience on the health of patients with MS, it is recommended to use resilience intervention programs for patients with MS.
Ethical Considerations
Compliance with ethical guidelines
At the beginning of the interview, the purpose of the study, and data confidentiality were explained to the participants and written and verbal consent were obtained. The subjects had the right to withdraw from the study at any time. The study has been approved by research committee of University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1401.083)
Funding
The present article was extracted from the master's thesis of Fatemeh Qadbigi, approved by Department of Social Work, School of Social Health, University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Conceptualization: Fardin Alipour; Design of study: Fatemeh Ghadbeigi and Fardin Alipour; Data collection: Fatemeh Ghadbeigi; Data analysis: Fatemeh Ghadbeigi and Gholamreza Ghaedamini Harouni; Formal analysis: Fardin Alipour; Revising the manuscript: Fardin Alipour and Zoleikha Arabkari; Reading and approving the final manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
Reference
- Atkins G, Amor S, Fletcher J, Mills K. The biology of multiple sclerosis. Cambridge: Cambridge University Press; 2012. [DOI:10.1017/CBO9780511979088]
- Hughes AJ, Patel K, Fitzgerald KC, Brown A, Gromisch ES, Mowry EM. Reliability and validity of the multiple sclerosis resiliency scale (MSRS). Journal of the Neurological Sciences. 2020 418:116983. [DOI:10.1016/j.jns.2020.116983] [PMID]
- Swank RL, Dugan BB. The multiple sclerosis diet book. New York: Knopf Doubleday Publishing Group; 2011. [Link]
- Olek M. Multiple sclerosis: Etiology, diagnosis, and new treatment strategies. Totowa: Humana Press; 2005. [Link]
- Iezzoni LI. Multiple sclerosis: ABC-CLIO. Santa Barbara: Greenwood; 2010. [DOI:10.5040/9798400688379]
- Gromisch ES, Sloan J, Zemon V, Tyry T, Schairer LC, Snyder S, et al. Development of the multiple sclerosis resiliency scale (MSRS). Rehabilitation Psychology. 2018; 63(3):357-64. [DOI:10.1037/rep0000219] [PMID]
- Hajmohammadi R, Shirazi M. Predicting resilience via social support and illness perceptions among patients undergoing Hemodialysis. Jundishapur Journal of Chronic Disease Care. 2017; 6(3):e14427. [DOI:10.5812/jjcdc.14427]
- Kashani VO, Dehestani F, Soltaniyan MA. [Validation of the Persian Version of Dynamic Gait Index in multiple sclerosis diseases (4-Item) (Persian)]. Motor Behavior. 2019; 11(35):117-32. [Link]
- Shahvaroughi FA, Azimian M, Falahpour M, Karimlou M. [Fatigue Severity Scale (FSS): Evaluatiopn of reliability of the Persian version among persons with multiple sclerosis (Persian)]. Archives of Rehabilitation. 2009; 10(4):47-51. [Link]
- Mohammadi K, Rahnama P, Montazeri A, Foley FW. The multiple sclerosis intimacy and sexuality questionnaire-19: Reliability, validity, and factor structure of the Persian version. The Journal of Sexual Medicine. 2014; 11(9):2225-31. [DOI:10.1111/jsm.12531]
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica. 1983; 67(6):361-70. [DOI:10.1111/j.1600-0447.1983.tb09716.x] [PMID]
- Kaviani H, Seyfourian H, Sharifi V, Ebrahimkhani N. [Reliability and validity of anxiety and depression hospital scales (HADS): Iranian patients with anxiety and depression disorders (Persian)]. Tehran University Medical Journal. 2009; 67(5):379-85. [Link]
- Neto L, Gromisch ES, Sloan J, Tyry T, Foley FW. The relationship between aspects of resiliency and intimacy-related illness intrusiveness in males with multiple sclerosis. Sexuality and Disability. 38:135-45. [DOI:10.1007/s11195-019-09609-z]
- Duan W, Mu W, Xiong H. Cross-cultural adaptation and validation of the physical disability resiliency scale in a sample of Chinese with physical disability. Frontiers in Psychology. 2020; 11:602736. [DOI:10.3389/fpsyg.2020.602736] [PMID] [PMCID]
- Schulz KH, Gold SM, Witte J, Bartsch K, Lang UE, Hellweg R, et al. Impact of aerobic training on immune-endocrine parameters, neurotrophic factors, quality of life and coordinative function in multiple sclerosis. Journal of the Neurological Sciences. 2004; 225(1-2):11-8. [DOI:10.1016/j.jns.2004.06.009] [PMID]
- Pakenham KI, Mawdsley M, Brown FL, Burton NW. Pilot evaluation of a resilience training program for people with multiple sclerosis. Rehabilitation Psychology. 2018; 63(1):29-42. [DOI:10.1037/rep0000167] [PMID]
- Kim S, Esquivel GB. Adolescent spirituality and resilience: Theory, research, and educational practices. Psychology in the Schools. 2011; 48(7):755-65. [DOI:10.1002/pits.20582
- Liśkiewicz A, Przybyła M, Wojakowska A, Marczak Ł, Bogus K, Nowacka-Chmielewska M, et al. Physical activity reduces anxiety and regulates brain fatty acid synthesis. Molecular Brain. 2020; 13(1):62. [DOI:10.1186/s13041-020-00592-7] [PMID] [PMCID]
- Ozkara AB, Kalkavan A, Alemdag S, Alemdag C. The role of physical activity in psychological resilience. Baltic Journal of Sport and Health Sciences. 2016; 3(102):24-9. [DOI:10.33607/bjshs.v3i102.62]
- Benard B. Resiliency: What we have learned. San Francisco: WestEd; 2004. [Link]
- Cohen JA, Rudick RA. (2011). Multiple sclerosis therapeutics. Cambridge: Cambridge University Press; 2011. [DOI:10.1017/CBO9781139023986]
- Peres JF, Moreira-Almeida A, Nasello AG, Koenig HG. Spirituality and resilience in trauma victims. Journal of Religion and Health. 2007; 46:343-50. [DOI:10.1007/s10943-006-9103-0]
Type of Study: Original |
Subject:
Social Worker
Received: 6/04/2023 | Accepted: 13/11/2023 | Published: 1/04/2024
Received: 6/04/2023 | Accepted: 13/11/2023 | Published: 1/04/2024
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Archives of Rehabilitation (RJ)
Journal Tel: +98 (21) 71732812, 09941095452 (Call time Saturday to Wednesday 8 to 14)
Publisher Tel: +9821 453 55 555 - 453 55 000
E-mail: rehabilitationjour@gmail.com
Archives of Rehabilitation (RJ)
Journal Tel: +98 (21) 71732812, 09941095452 (Call time Saturday to Wednesday 8 to 14)
Publisher Tel: +9821 453 55 555 - 453 55 000
E-mail: rehabilitationjour@gmail.com
