

Volume 24, Issue 4 (Winter 2024)
jrehab 2024, 24(4): 586-601 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Razi Sangtabi N, Khalkhali Zavieh M, Khademi Kalantari K, Ghandali E, Akbarzadeh Baghban A. Studying the Effect of Cross-education on the Quadriceps Atherogenic Muscle Inhibition in Women With Unilateral Knee Osteoarthritis. jrehab 2024; 24 (4) :586-601
URL: http://rehabilitationj.uswr.ac.ir/article-1-3257-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3257-en.html
Nastaran Razi Sangtabi1 

 , Minoo Khalkhali Zavieh *2 , Khosro Khademi Kalantari3 , Elham Ghandali3 , Alireza Akbarzadeh Baghban4
, Minoo Khalkhali Zavieh *2 , Khosro Khademi Kalantari3 , Elham Ghandali3 , Alireza Akbarzadeh Baghban4
, Minoo Khalkhali Zavieh *2 , Khosro Khademi Kalantari3 , Elham Ghandali3 , Alireza Akbarzadeh Baghban4
1- Department of Physiotherapy, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Physiotherapy Research Center, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,minoo_kh@yahoo.com
3- Physiotherapy Research Center, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran., Department of Physiotherapy, Faculty of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Department of Biostatistics, Proteomics Research Center, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Physiotherapy Research Center, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,
3- Physiotherapy Research Center, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran., Department of Physiotherapy, Faculty of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Department of Biostatistics, Proteomics Research Center, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 1658 kb]
(737 Downloads)
| Abstract (HTML) (5906 Views)
Full-Text: (1073 Views)
Introduction
Osteoarthritis (OA) of the knee is the most common degenerative joint disease [1]. The characteristics of this disease include the destruction of the joint surface, and reduction of joint space, resulting in pain and swelling, which declines muscle strength and quality of life [2، 3]. This joint destruction is common in people over 50 [4]. Quadriceps muscle weakness is a common clinical symptom associated with pain and physical disability caused by knee OA [3، 5].
Atherogenic muscle inhibition (AMI) is one of the causes of quadriceps muscle weakness, which is usually observed in patients with OA and prevents the maximum activation of this muscle [6]. AMI in OA results from pain and progressive destruction of the joint [7]. In this scenario, following the damage to the joint, the muscles around the joint are reflexively inhibited, even if they have not been damaged [8]. Atherogenic inhibition of the quadriceps muscle is one of the therapist’s concerns, which causes muscle weakness, atrophy in the healed joint [9], and prevention of effective muscle strengthening [8]. There is much evidence regarding the effectiveness of exercise therapy for treating knee OA symptoms [10]. Therefore, treatments that improve the quadriceps muscle strength in people with knee OA are necessary. However, these patients cannot perform strength exercises in the affected limb due to pain and AMI. This condition prevents the increase in effective muscle strength and makes it difficult to use it in the rehabilitation program. It is believed that the strong contraction of the muscles around the inflamed joint can cause damage to that muscle [12].
From a clinical point of view, the persistence of muscle weakness can be of concern due to defects in the dynamic stability of the knee joint [13], physical performance [14], and increasing pressure on the knee joint [15]. Cross-education (CE) is a therapeutic method to increase the strength of the muscles of the involved limb without exercising the involved limb. Strength training in one limb increases muscle strength in the opposite limb (the limb not subjected to exercise treatment) [16]. Lipley et al. investigated the effect of 24 sessions of CE on the strength and activity of the quadriceps muscle in healthy individuals. Their findings reported an improvement in the eccentric strength of the quadriceps muscle in the opposite limb (the limb on which the exercise was not performed) [17]. Onigbinde et al. investigated the effect of CE in people with knee OA. They reported that after 6 weeks of isometric training on the healthy limb, the maximum isometric strength of the quadriceps muscle in the limb with OA increased significantly [18]. It is unclear how the decrease in AMI can increase muscle strength.
This study investigates the effect of one session of CE on AMI and maximum extensor torque of the quadriceps muscle in women with unilateral knee OA. The results of which can clarify the possible mechanism of CE in these patients.
Material and Methods
Study participants
In this quasi-experimental study, 21 women with unilateral knee OA were included based on the inclusion and exclusion criteria after getting familiarized with the study process and completing the informed consent form. These women had grade 2 knee OA based on the Kellgren-Lawrence grading scale.
The exclusion criteria included Suffering from severe cardiovascular diseases, history of surgery or arthroplasty in the lower limb, history of rheumatic and infectious diseases in the knee, history of cancer, and inability to give information and use drugs.
Study procedure
In this study, the amount of atherogenic inhibition and the maximum extensor torque in the quadriceps muscle of the knee affected by OA were measured in 3 stages: 1) Before the CE, 2) Immediately after the CE, and 3) 15 minutes after the CE.
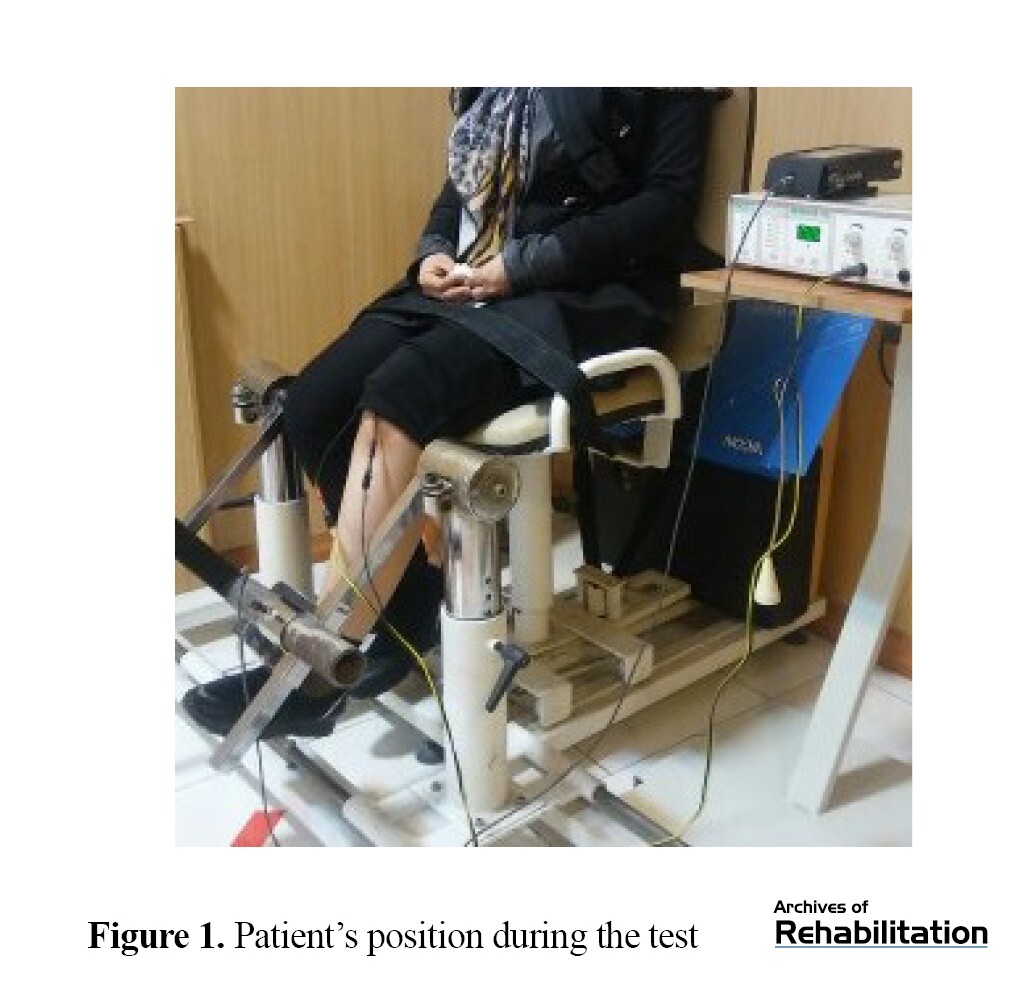
Measurement of atherogenic inhibition and maximum extensor torque in the quadriceps muscle were as follows. A dynamometer connected to an 8-channel Data log (Data log, Biometrics, UK) was used to record the maximum extensor torque of the quadriceps muscle of the knee with OA. The locations of the electrodes were determined according to surface electromyography for the non-invasive assessment of muscles (SENIAM) criteria [19]. Before testing, each subject performed 20 sub-maximal contractions while sitting on a chair (Figure 1) to warm up the quadriceps muscle and get more familiar with the test conditions.
After that, the patient was asked to make her maximum voluntary effort to activate the quadriceps muscle by pressing on the dynamometer installed on the chair. After 3 seconds of contraction, the electrical stimulation of the quadriceps muscle was applied to the individual’s maximum voluntary effort (burst superimposition). This contraction also lasted for 3 seconds. The electrical stimulation device used in this study was a 2-channel device with a current frequency of 40 Hz. To electrically stimulate the quadriceps muscle, we used one electrode on the muscle block and another electrode about 2 cm distal to it (according to SENIAM criteria) [19].
The atherogenic inhibition of the quadriceps muscle of the knee affected by osteoarthritis was calculated using the maximal activation defect formula (Equation 1) [20]. The measurement of atherogenic inhibition was performed 3 times with an interval of 2 minutes each time. The average of the 3 measurements was considered the amount of atherogenic inhibition of the quadriceps muscle.

Treatment
In cross-education, the patient was asked to make a maximum voluntary effort to activate the quadriceps muscle of the asymptomatic knee isometrically by pressing on the pad installed on the chair. The exercise was done in 5 sets, each set including 8 contractions.
Data analysis
Based on the one-sample Kolmogorov-Smirnov (K-S) test results, the variables of atherogenic inhibition of the quadriceps muscle and maximum extensor torque had a normal distribution. Therefore, the comparison was made in three measurement times with the help of repeated measures analysis of variance (ANOVA) test. The significance level was considered <0.05.
Results
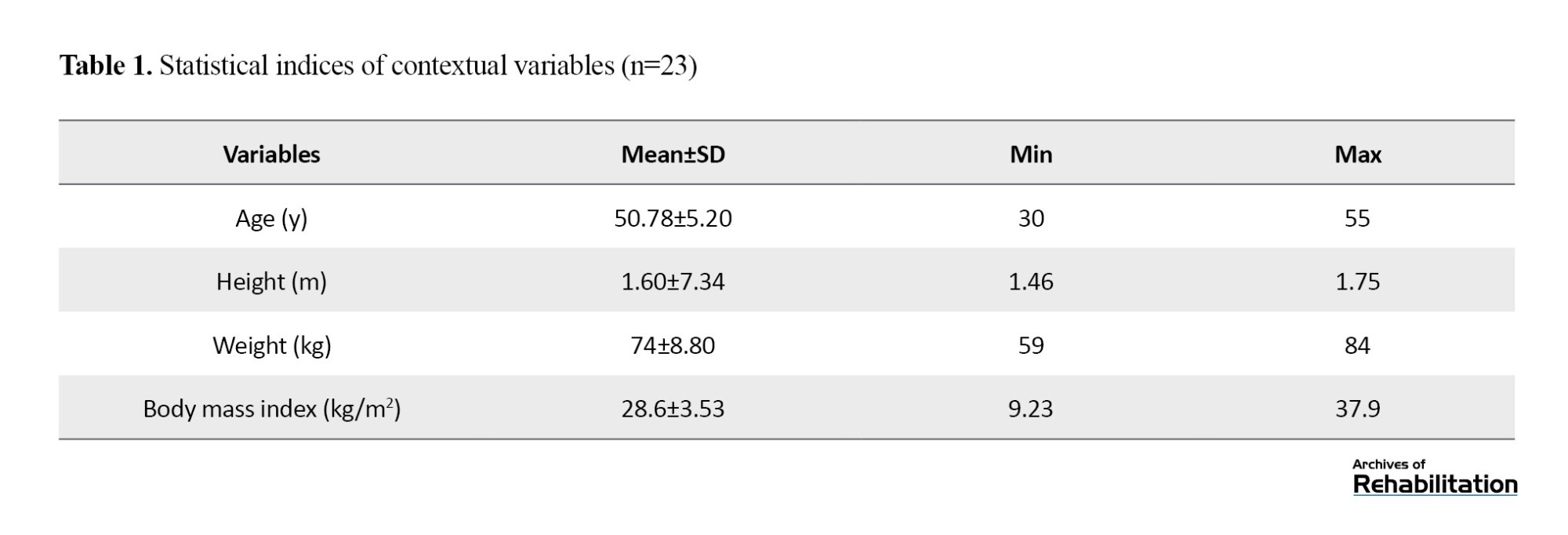
Descriptive statistics (Mean±SD) of demographic characteristics, including height (measured with a tape measure), weight (measured with a scale), age, and body mass index (BMI) are presented in Table 1.
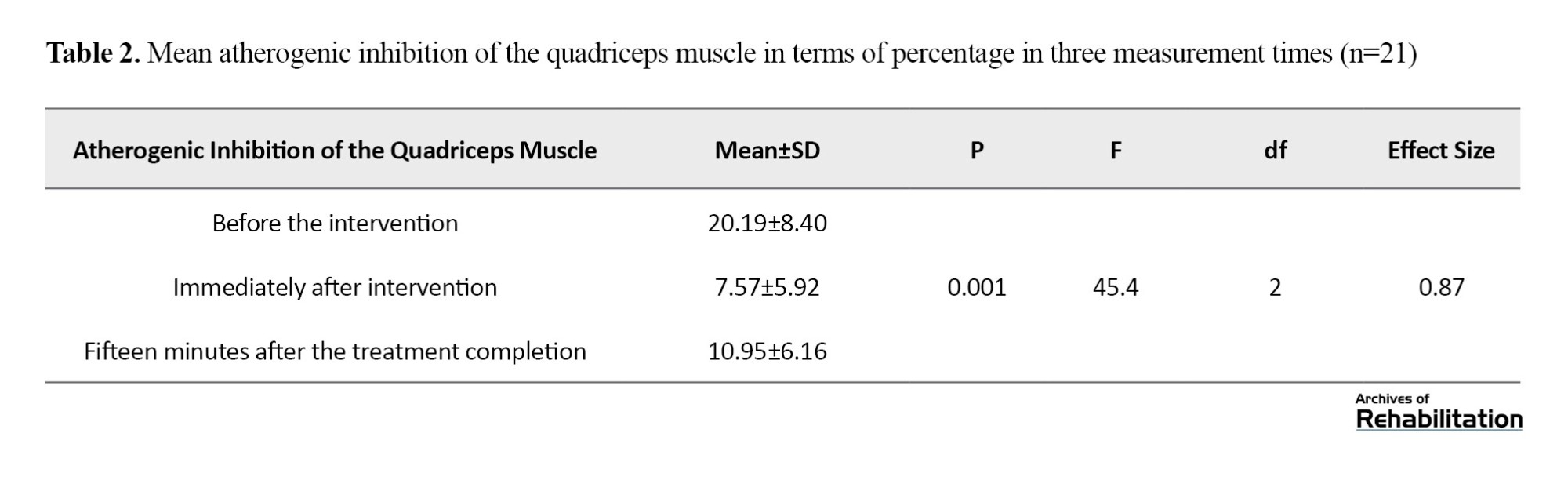
According to the K-S test, the atherogenic inhibition variables of the quadriceps muscle and the maximum extensor torque had a normal distribution. Repeated measures ANOVA showed that the atherogenic inhibition rate of the quadriceps muscle after cross-training was significantly lower than that before the intervention (P=0.001). Although the amount of atherogenic inhibition of the quadriceps muscle has increased compared to the time immediately after the intervention, it is still significantly (P=0.001) lower than that before the intervention (Table 2).
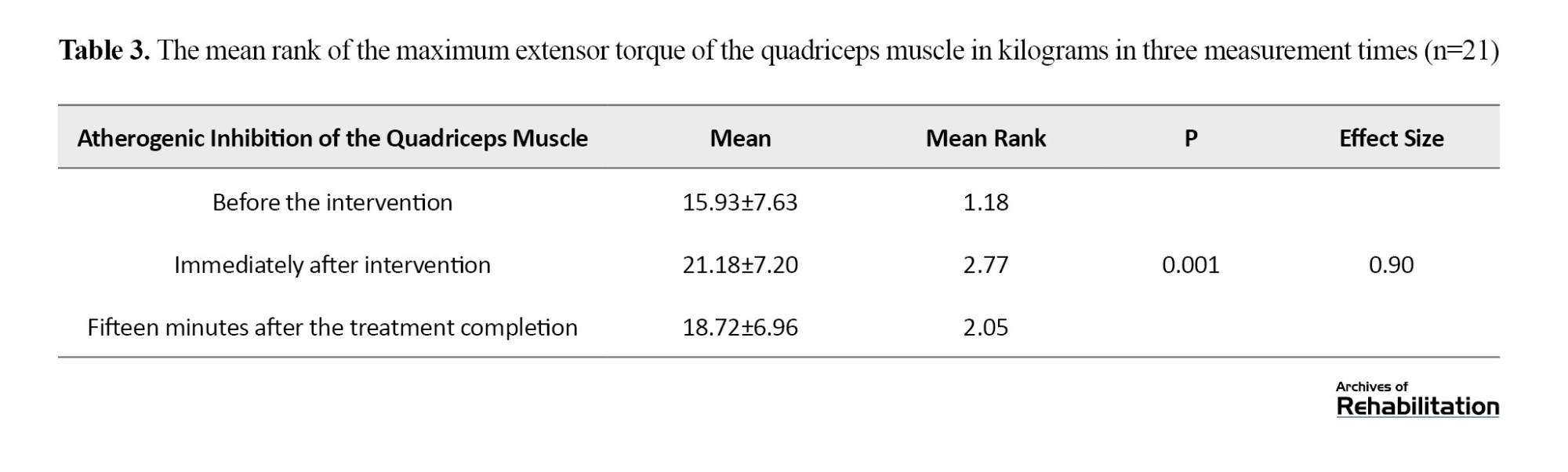
According to the results, the maximum extensor torque of the quadriceps muscle after CE was significantly higher than that before the intervention (P=0.001). Although the maximum extensor torque of the quadriceps muscle decreased 15 minutes after the end of the intervention compared to the time immediately after the intervention, it was still significantly higher (P=0.001) than that before the intervention (Table 3).
Using the Bonferroni test, the pairwise comparison showed that the average atherogenic inhibition of the quadriceps muscle immediately after the intervention and 15 minutes after its completion was significantly lower than before the intervention (P=0.001). Also, the average atherogenic inhibition increased significantly 15 minutes after the end of the intervention, compared to immediately after the intervention (P=0.018).
In addition, the results of the maximum extensor torque of the quadriceps muscle immediately after the intervention and 15 minutes after its completion showed a significant increase compared to before the intervention (P<0.001). Still, it significantly reduced 15 minutes after the end of the intervention compared to the time immediately after the intervention (P<0.001).
Discussion
The results of the present study showed that one session of CE significantly reduced atherogenic inhibition and increased the maximum extensor torque in the quadriceps muscle of women with knee OA. Atherogenic inhibition in people with knee OA can be caused by the progressive destruction of the joint and abnormal joint afferent messages to α motor neurons and the subsequent decrease in the activity of these neurons, which causes a defect in the central nervous system to activate the muscle voluntarily and completely. This condition is common among patients with knee OA and can lead to functional defects caused by the progress of the disease [7، 21].
Onigbinde et al.’s study (2017) showed an increase in the maximum extensor torque of the quadriceps muscle after 6 weeks of isometric CE training in people with knee OA. However, the effect of CE on the atherogenic inhibition of the quadriceps muscle was not investigated in these people. The results showed that CE, while performed only on the non-involved limb, causes therapeutic effects on the involved limb [18]. Lepley’s study investigated the effect of CE on the maximum activation defect of the quadriceps muscle in healthy individuals, and its results were not clinically significant [17]. The sample size in this study was small (n=9), and maximal activation defect was investigated in healthy people, which is much less compared to atherogenic inhibition in people with knee OA. The present study showed that performing one CE session significantly reduces atherogenic inhibition and increases the maximum extensor torque of the quadriceps muscle in women with knee OA. The neural mechanism is one of the most important mechanisms proposed for the CE effect. According to the evidence, the structure and organization of the brain, including the anatomical connections between the two hemispheres, play an important role in this phenomenon. Unilateral resistance exercises in one limb change the organization of movement pathways that control the muscles of the opposite side [22].
Voluntary unilateral contractions with high force change the excitability of cortical neural pathways that go to the opposite side [22]. This condition can be caused by the reduction of transcallosal inhibition between the two primary motor cortices after mutual training [23]. In addition, strong contractions in one limb can affect the cortex of the same side and cause adaptations in the control system of the opposite side that cause more effective motor afferents to the opposite limb without training when maximally contracted [24]. All these events are due to the connections between the two primary motor cortexes and the premotor area’s connections with the primary motor cortex [25]. Studies using transcranial magnetic stimulation have shown that brain afferents from the motor cortex to untrained muscles increase during unilateral resistance training. Also, brain-spinal excitability rises in both the trained and untrained hemispheres [26]. In addition, interhemispheric inhibition during activity is reduced in the limb without training, which suggests the plasticity of interhemispheric connections to create the CE phenomenon [27]. Studies that have investigated the activity of the motor cortex of the opposite limb without training during training to the other side have shown an increase in the activity in the motor cortex of the opposite limb [28].
Conclusion
The results of this study showed that one session of CE training can decrease atherogenic inhibition, followed by an increase in the maximum extensor torque of the quadriceps muscle in women with unilateral knee OA. Also, the effects remain until 15 minutes after the end of the exercise. However, this study did not examine the long-term effects of these exercises. It will be clinically important if future studies show the long-term effects of these exercises. In cases such as OA of the knee or other injuries, where due to pain or reasons such as fear of further damage or disrupting the healing process, we cannot perform strengthening exercises in the quadriceps muscle of the affected knee directly, the degree of atherogenic inhibition in the knee increases and remains for a longer period. This condition leads to the difficulty of the rehabilitation process of these patients and makes it useless to perform strengthening exercises in the injured knee. In these cases, it is possible to reduce the atherogenic inhibition and increase the maximum extensor torque of the quadriceps muscle of the affected knee by performing strengthening exercises in the quadriceps muscle of the asymptomatic knee without engaging the affected limb and causing more damage to it. By reducing atherogenic inhibition, the patient can perform strengthening exercises more effectively in the quadriceps muscle, which is one of the most important parts of the rehabilitation program in such patients. This condition will probably lead to strengthening these muscles and improving knee function after injury.
According to the current study’s results, CE based on neural adaptations will decrease atherogenic inhibition in the quadriceps muscle of the knee with OA, which can be a reason for increasing the maximum extensor torque of the quadriceps muscle in these people. However, it should be noted that the long-term effects of these exercises have not been investigated in this study, and there is a need to examine it from a clinical point of view in future studies.
CE becomes important when people with OA of the knee or other joint injuries due to various reasons such as pain, fear of further damage, disruption in the process of tissue repair, and prohibition of strengthening exercises in the affected knee and other reasons, are unable to perform strengthening exercises in the quadriceps muscle of the injured knee. Conducting more studies and clarifying the nature and mechanism of CE effect on atherogenic inhibition can further help use this method in skeletal-muscular injuries.
Ethical Considerations
Compliance with ethical guidelines
The present article was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences with ID IR.SBMU.RETECH.REC.1397.1194. Written consent was obtained from the participants and their legal guardians to participate in the research. All participants took part in the current study with their consent, and there was no coercion or pressure to convince them to participate. The participants completed the written informed consent form and had the right to withdraw from the research. Also, the patients and their legal guardians were informed that all information would remain confidential and no one would disclose it unless the patients and their guardians requested it. In this research, an attempt was made to avoid harming the patients.
Funding
This article is taken from the master’s thesis of Nastaran Razi Sangtabi, approved by Department of Physiotherapy, School of Rehabilitation, Shahid Beheshti University of Medical Sciences.
Authors' contributions
Conceptualization and supervision: Minoo Khalkhali Zaviye and Khosro Khademi Kalantari; Methodology and validation: Nastaran Razi Sangtabi, Minoo Khalkhali Zaviye, and Khosro Khademi Kalantari; Visualization: Elham Kandali; Analysis: Khosro Khademi Kalantari and Alireza Akbarzadeh Baghban; Research and review: Nastaran Razi Sangtabi and Elham Kandali; Sources: Nastaran Razi Sangtabi and Minoo Khalkhali Zaviye; Writing the original draft: Nastaran Razi Sangtabi; Review, editing and final approval: Elham Qandali and Khosro Khademi Kalantari.
Conflict of interest
All authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the personnel and officials of the Physiotherapy Clinic of Shahid Beheshti University of Medical Sciences who prepared the preparations for this research.
Osteoarthritis (OA) of the knee is the most common degenerative joint disease [1]. The characteristics of this disease include the destruction of the joint surface, and reduction of joint space, resulting in pain and swelling, which declines muscle strength and quality of life [2، 3]. This joint destruction is common in people over 50 [4]. Quadriceps muscle weakness is a common clinical symptom associated with pain and physical disability caused by knee OA [3، 5].
Atherogenic muscle inhibition (AMI) is one of the causes of quadriceps muscle weakness, which is usually observed in patients with OA and prevents the maximum activation of this muscle [6]. AMI in OA results from pain and progressive destruction of the joint [7]. In this scenario, following the damage to the joint, the muscles around the joint are reflexively inhibited, even if they have not been damaged [8]. Atherogenic inhibition of the quadriceps muscle is one of the therapist’s concerns, which causes muscle weakness, atrophy in the healed joint [9], and prevention of effective muscle strengthening [8]. There is much evidence regarding the effectiveness of exercise therapy for treating knee OA symptoms [10]. Therefore, treatments that improve the quadriceps muscle strength in people with knee OA are necessary. However, these patients cannot perform strength exercises in the affected limb due to pain and AMI. This condition prevents the increase in effective muscle strength and makes it difficult to use it in the rehabilitation program. It is believed that the strong contraction of the muscles around the inflamed joint can cause damage to that muscle [12].
From a clinical point of view, the persistence of muscle weakness can be of concern due to defects in the dynamic stability of the knee joint [13], physical performance [14], and increasing pressure on the knee joint [15]. Cross-education (CE) is a therapeutic method to increase the strength of the muscles of the involved limb without exercising the involved limb. Strength training in one limb increases muscle strength in the opposite limb (the limb not subjected to exercise treatment) [16]. Lipley et al. investigated the effect of 24 sessions of CE on the strength and activity of the quadriceps muscle in healthy individuals. Their findings reported an improvement in the eccentric strength of the quadriceps muscle in the opposite limb (the limb on which the exercise was not performed) [17]. Onigbinde et al. investigated the effect of CE in people with knee OA. They reported that after 6 weeks of isometric training on the healthy limb, the maximum isometric strength of the quadriceps muscle in the limb with OA increased significantly [18]. It is unclear how the decrease in AMI can increase muscle strength.
This study investigates the effect of one session of CE on AMI and maximum extensor torque of the quadriceps muscle in women with unilateral knee OA. The results of which can clarify the possible mechanism of CE in these patients.
Material and Methods
Study participants
In this quasi-experimental study, 21 women with unilateral knee OA were included based on the inclusion and exclusion criteria after getting familiarized with the study process and completing the informed consent form. These women had grade 2 knee OA based on the Kellgren-Lawrence grading scale.
The exclusion criteria included Suffering from severe cardiovascular diseases, history of surgery or arthroplasty in the lower limb, history of rheumatic and infectious diseases in the knee, history of cancer, and inability to give information and use drugs.
Study procedure
In this study, the amount of atherogenic inhibition and the maximum extensor torque in the quadriceps muscle of the knee affected by OA were measured in 3 stages: 1) Before the CE, 2) Immediately after the CE, and 3) 15 minutes after the CE.
Measurement of atherogenic inhibition and maximum extensor torque in the quadriceps muscle were as follows. A dynamometer connected to an 8-channel Data log (Data log, Biometrics, UK) was used to record the maximum extensor torque of the quadriceps muscle of the knee with OA. The locations of the electrodes were determined according to surface electromyography for the non-invasive assessment of muscles (SENIAM) criteria [19]. Before testing, each subject performed 20 sub-maximal contractions while sitting on a chair (Figure 1) to warm up the quadriceps muscle and get more familiar with the test conditions.
After that, the patient was asked to make her maximum voluntary effort to activate the quadriceps muscle by pressing on the dynamometer installed on the chair. After 3 seconds of contraction, the electrical stimulation of the quadriceps muscle was applied to the individual’s maximum voluntary effort (burst superimposition). This contraction also lasted for 3 seconds. The electrical stimulation device used in this study was a 2-channel device with a current frequency of 40 Hz. To electrically stimulate the quadriceps muscle, we used one electrode on the muscle block and another electrode about 2 cm distal to it (according to SENIAM criteria) [19].
The atherogenic inhibition of the quadriceps muscle of the knee affected by osteoarthritis was calculated using the maximal activation defect formula (Equation 1) [20]. The measurement of atherogenic inhibition was performed 3 times with an interval of 2 minutes each time. The average of the 3 measurements was considered the amount of atherogenic inhibition of the quadriceps muscle.
Treatment
In cross-education, the patient was asked to make a maximum voluntary effort to activate the quadriceps muscle of the asymptomatic knee isometrically by pressing on the pad installed on the chair. The exercise was done in 5 sets, each set including 8 contractions.
Data analysis
Based on the one-sample Kolmogorov-Smirnov (K-S) test results, the variables of atherogenic inhibition of the quadriceps muscle and maximum extensor torque had a normal distribution. Therefore, the comparison was made in three measurement times with the help of repeated measures analysis of variance (ANOVA) test. The significance level was considered <0.05.
Results
Descriptive statistics (Mean±SD) of demographic characteristics, including height (measured with a tape measure), weight (measured with a scale), age, and body mass index (BMI) are presented in Table 1.
According to the K-S test, the atherogenic inhibition variables of the quadriceps muscle and the maximum extensor torque had a normal distribution. Repeated measures ANOVA showed that the atherogenic inhibition rate of the quadriceps muscle after cross-training was significantly lower than that before the intervention (P=0.001). Although the amount of atherogenic inhibition of the quadriceps muscle has increased compared to the time immediately after the intervention, it is still significantly (P=0.001) lower than that before the intervention (Table 2).
According to the results, the maximum extensor torque of the quadriceps muscle after CE was significantly higher than that before the intervention (P=0.001). Although the maximum extensor torque of the quadriceps muscle decreased 15 minutes after the end of the intervention compared to the time immediately after the intervention, it was still significantly higher (P=0.001) than that before the intervention (Table 3).
Using the Bonferroni test, the pairwise comparison showed that the average atherogenic inhibition of the quadriceps muscle immediately after the intervention and 15 minutes after its completion was significantly lower than before the intervention (P=0.001). Also, the average atherogenic inhibition increased significantly 15 minutes after the end of the intervention, compared to immediately after the intervention (P=0.018).
In addition, the results of the maximum extensor torque of the quadriceps muscle immediately after the intervention and 15 minutes after its completion showed a significant increase compared to before the intervention (P<0.001). Still, it significantly reduced 15 minutes after the end of the intervention compared to the time immediately after the intervention (P<0.001).
Discussion
The results of the present study showed that one session of CE significantly reduced atherogenic inhibition and increased the maximum extensor torque in the quadriceps muscle of women with knee OA. Atherogenic inhibition in people with knee OA can be caused by the progressive destruction of the joint and abnormal joint afferent messages to α motor neurons and the subsequent decrease in the activity of these neurons, which causes a defect in the central nervous system to activate the muscle voluntarily and completely. This condition is common among patients with knee OA and can lead to functional defects caused by the progress of the disease [7، 21].
Onigbinde et al.’s study (2017) showed an increase in the maximum extensor torque of the quadriceps muscle after 6 weeks of isometric CE training in people with knee OA. However, the effect of CE on the atherogenic inhibition of the quadriceps muscle was not investigated in these people. The results showed that CE, while performed only on the non-involved limb, causes therapeutic effects on the involved limb [18]. Lepley’s study investigated the effect of CE on the maximum activation defect of the quadriceps muscle in healthy individuals, and its results were not clinically significant [17]. The sample size in this study was small (n=9), and maximal activation defect was investigated in healthy people, which is much less compared to atherogenic inhibition in people with knee OA. The present study showed that performing one CE session significantly reduces atherogenic inhibition and increases the maximum extensor torque of the quadriceps muscle in women with knee OA. The neural mechanism is one of the most important mechanisms proposed for the CE effect. According to the evidence, the structure and organization of the brain, including the anatomical connections between the two hemispheres, play an important role in this phenomenon. Unilateral resistance exercises in one limb change the organization of movement pathways that control the muscles of the opposite side [22].
Voluntary unilateral contractions with high force change the excitability of cortical neural pathways that go to the opposite side [22]. This condition can be caused by the reduction of transcallosal inhibition between the two primary motor cortices after mutual training [23]. In addition, strong contractions in one limb can affect the cortex of the same side and cause adaptations in the control system of the opposite side that cause more effective motor afferents to the opposite limb without training when maximally contracted [24]. All these events are due to the connections between the two primary motor cortexes and the premotor area’s connections with the primary motor cortex [25]. Studies using transcranial magnetic stimulation have shown that brain afferents from the motor cortex to untrained muscles increase during unilateral resistance training. Also, brain-spinal excitability rises in both the trained and untrained hemispheres [26]. In addition, interhemispheric inhibition during activity is reduced in the limb without training, which suggests the plasticity of interhemispheric connections to create the CE phenomenon [27]. Studies that have investigated the activity of the motor cortex of the opposite limb without training during training to the other side have shown an increase in the activity in the motor cortex of the opposite limb [28].
Conclusion
The results of this study showed that one session of CE training can decrease atherogenic inhibition, followed by an increase in the maximum extensor torque of the quadriceps muscle in women with unilateral knee OA. Also, the effects remain until 15 minutes after the end of the exercise. However, this study did not examine the long-term effects of these exercises. It will be clinically important if future studies show the long-term effects of these exercises. In cases such as OA of the knee or other injuries, where due to pain or reasons such as fear of further damage or disrupting the healing process, we cannot perform strengthening exercises in the quadriceps muscle of the affected knee directly, the degree of atherogenic inhibition in the knee increases and remains for a longer period. This condition leads to the difficulty of the rehabilitation process of these patients and makes it useless to perform strengthening exercises in the injured knee. In these cases, it is possible to reduce the atherogenic inhibition and increase the maximum extensor torque of the quadriceps muscle of the affected knee by performing strengthening exercises in the quadriceps muscle of the asymptomatic knee without engaging the affected limb and causing more damage to it. By reducing atherogenic inhibition, the patient can perform strengthening exercises more effectively in the quadriceps muscle, which is one of the most important parts of the rehabilitation program in such patients. This condition will probably lead to strengthening these muscles and improving knee function after injury.
According to the current study’s results, CE based on neural adaptations will decrease atherogenic inhibition in the quadriceps muscle of the knee with OA, which can be a reason for increasing the maximum extensor torque of the quadriceps muscle in these people. However, it should be noted that the long-term effects of these exercises have not been investigated in this study, and there is a need to examine it from a clinical point of view in future studies.
CE becomes important when people with OA of the knee or other joint injuries due to various reasons such as pain, fear of further damage, disruption in the process of tissue repair, and prohibition of strengthening exercises in the affected knee and other reasons, are unable to perform strengthening exercises in the quadriceps muscle of the injured knee. Conducting more studies and clarifying the nature and mechanism of CE effect on atherogenic inhibition can further help use this method in skeletal-muscular injuries.
Ethical Considerations
Compliance with ethical guidelines
The present article was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences with ID IR.SBMU.RETECH.REC.1397.1194. Written consent was obtained from the participants and their legal guardians to participate in the research. All participants took part in the current study with their consent, and there was no coercion or pressure to convince them to participate. The participants completed the written informed consent form and had the right to withdraw from the research. Also, the patients and their legal guardians were informed that all information would remain confidential and no one would disclose it unless the patients and their guardians requested it. In this research, an attempt was made to avoid harming the patients.
Funding
This article is taken from the master’s thesis of Nastaran Razi Sangtabi, approved by Department of Physiotherapy, School of Rehabilitation, Shahid Beheshti University of Medical Sciences.
Authors' contributions
Conceptualization and supervision: Minoo Khalkhali Zaviye and Khosro Khademi Kalantari; Methodology and validation: Nastaran Razi Sangtabi, Minoo Khalkhali Zaviye, and Khosro Khademi Kalantari; Visualization: Elham Kandali; Analysis: Khosro Khademi Kalantari and Alireza Akbarzadeh Baghban; Research and review: Nastaran Razi Sangtabi and Elham Kandali; Sources: Nastaran Razi Sangtabi and Minoo Khalkhali Zaviye; Writing the original draft: Nastaran Razi Sangtabi; Review, editing and final approval: Elham Qandali and Khosro Khademi Kalantari.
Conflict of interest
All authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the personnel and officials of the Physiotherapy Clinic of Shahid Beheshti University of Medical Sciences who prepared the preparations for this research.
References
- Kan HS, Chan PK, Chiu KY, Yan CH, Yeung SS, Ng YL, et al. Non-surgical treatment of knee osteoarthritis. Hong Kong Medical Journal. 2019; 25(2):127-33. [DOI:10.12809/hkmj187600] [PMID]
- Scott D, Kowalczyk A. Osteoarthritis of the knee. BMJ Clinical Evidence. 2007; 2007:1121. [PMID] [PMCID]
- Palmieri-Smith RM, Thomas AC, Karvonen-Gutierrez C, Sowers MF. Isometric quadriceps strength in women with mild, moderate, and severe knee osteoarthritis. American Journal of Physical Medicine & Rehabilitation. 2010; 89(7):541-8. [DOI:10.1097/PHM.0b013e3181ddd5c3] [PMID] [PMCID]
- Bruyère O, Honvo G, Veronese N, Arden NK, Branco J, Curtis EM, et al. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Seminars in Arthritis and Rheumatism. 2019; 49(3):337-50. [DOI:10.1016/j.semarthrit.2019.04.008] [PMID]
- Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: An update with relevance for clinical practice. Lancet. 2011; 377(9783):2115-26. [DOI:10.1016/S0140-6736(11)60243-2] [PMID]
- Rice DA, McNair PJ. Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Seminars in Arthritis and Rheumatism. 2010; 40(3):250-66. [DOI:10.1016/j.semarthrit.2009.10.001] [PMID]
- Hurley MV, Scott DL, Rees J, Newham DJ. Sensorimotor changes and functional performance in patients with knee osteoarthritis. Annals of the Rheumatic Diseases. 1997; 56(11):641-8. [DOI:10.1136/ard.56.11.641] [PMID]
- Hopkins JT, Ingersoll CD. Arthrogenic muscle inhibition: A limiting factor in joint rehabilitation. Journal of Sport Rehabilitation. 2000; 9(2):135-59. [DOI:10.1123/jsr.9.2.135]
- Norte G, Rush J, Sherman D. Arthrogenic muscle inhibition: best evidence, mechanisms, and theory for treating the unseen in clinical rehabilitation. Journal of Sport Rehabilitation. 2021; 31(6):717-35. [DOI:10.1123/jsr.2021-0139] [PMID]
- Sharma L, Cahue S, Song J, Hayes K, Pai YC, Dunlop D. Physical functioning over three years in knee osteoarthritis: role of psychosocial, local mechanical, and neuromuscular factors. Arthritis and Rheumatism. 2003; 48(12):3359-70. [DOI:10.1002/art.11420] [PMID]
- Zhang W, Nuki G, Moskowitz RW, Abramson S, Altman RD, Arden NK, et al. OARSI recommendations for the management of hip and knee osteoarthritis: Part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis and Cartilage. 2010; 18(4):476-99. [DOI:10.1016/j.joca.2010.01.013] [PMID]
- Bodamyali T, Stevens CR, Billingham ME, Ohta S, Blake DR. Influence of hypoxia in inflammatory synovitis. Annals of The Rheumatic Diseases. 1998; 57(12):703-10. [DOI:10.1136/ard.57.12.703] [PMID]
- Felson DT, Niu J, McClennan C, Sack B, Aliabadi P, Hunter DJ, et al. Knee buckling: Prevalence, risk factors, and associated limitations in function. Annals of Internal Medicine. 2007; 147(8):534-40. [DOI:10.7326/0003-4819-147-8-200710160-00005] [PMID]
- Liikavainio T, Lyytinen T, Tyrväinen E, Sipilä S, Arokoski JP. Physical function and properties of quadriceps femoris muscle in men with knee osteoarthritis. Archives of Physical Medicine and Rehabilitation. 2008; 89(11):2185-94. [DOI:10.1016/j.apmr.2008.04.012] [PMID]
- Mikesky AE, Meyer A, Thompson KL. Relationship between quadriceps strength and rate of loading during gait in women. Journal of Orthopaedic Research. 2000; 18(2):171-5. [DOI:10.1002/jor.1100180202] [PMID]
- Scripture E, Smith TL, Brown EM. On the education of muscular control and power. Studies from The Yale Psychological Laboratory. 1894; 2(5):114-19. [Link]
- Lepley LK, Palmieri-Smith RM. Cross-education strength and activation after eccentric exercise. Journal of Athletic Training. 2014; 49(5):582-9. [DOI:10.4085/1062-6050-49.3.24] [PMID]
- Onigbinde AT, Ajiboye RA, Bada AI, Isaac SO. Inter-limb effects of isometric quadriceps strengthening on untrained contra-lateral homologous muscle of patients with knee osteoarthritis. Technology and Health Care. 2017; 25(1):19-27. [DOI:10.3233/THC-161239] [PMID]
- Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. Journal of Electromyography and Kinesiology. 2000; 10(5):361-74. [DOI:10.1016/S1050-6411(00)00027-4] [PMID]
- Rafsanjani H, Khademi-Kalantari K, Rezasoltani A, Naimi SS, Ghasemi M, Jaberzadeh S. Immediate effect of common peroneal nerve electrical stimulation on quadriceps muscle arthrogenic inhibition in patients with knee osteoarthritis. Journal of Bodywork and Movement Therapies. 2017; 21(4):879-83. [DOI:10.1016/j.jbmt.2017.03.003] [PMID]
- Hurley MV. The role of muscle weakness in the pathogenesis of osteoarthritis. Rheumatic Diseases Clinics of North America. 1999; 25(2):283-98. [DOI:10.1016/S0889-857X(05)70068-5] [PMID]
- Hortobágyi T, Taylor JL, Petersen NT, Russell G, Gandevia SC. Changes in segmental and motor cortical output with contralateral muscle contractions and altered sensory inputs in humans. Journal of Neurophysiology. 2003; 90(4):2451-9. [DOI:10.1152/jn.01001.2002] [PMID]
- Lee M, Carroll TJ. Cross education: Possible mechanisms for the contralateral effects of unilateral resistance training. Sports Medicine. 2007; 37(1):1-14. [DOI:10.2165/00007256-200737010-00001] [PMID]
- Carroll TJ, Herbert RD, Munn J, Lee M, Gandevia SC. Contralateral effects of unilateral strength training: Evidence and possible mechanisms. Journal of Applied Physiology. 2006; 101(5):1514-22. [DOI:10.1152/japplphysiol.00531.2006] [PMID]
- Mochizuki H, Huang YZ, Rothwell JC. Interhemispheric interaction between human dorsal premotor and contralateral primary motor cortex. The Journal of Physiology. 2004; 561(Pt 1):331-8. [DOI:10.1113/jphysiol.2004.072843] [PMID]
- Lee M, Gandevia SC, Carroll TJ. Unilateral strength training increases voluntary activation of the opposite untrained limb. Clinical Neurophysiology. 2009; 120(4):802-8. [DOI:10.1016/j.clinph.2009.01.002] [PMID]
- Hortobágyi T, Richardson SP, Lomarev M, Shamim E, Meunier S, Russman H, et al. Interhemispheric plasticity in humans. Medicine and Science in Sports and Exercise. 2011; 43(7):1188-99. [DOI:10.1249/MSS.0b013e31820a94b8] [PMID]
- Farthing JP, Krentz JR, Magnus CR, Barss TS, Lanovaz JL, Cummine J, et al. Changes in functional magnetic resonance imaging cortical activation with cross education to an immobilized limb. Medicine and Science in Sports and Exercise. 2011; 43(8):1394-405. [DOI:10.1249/MSS.0b013e318210783c] [PMID]
Type of Study: Original |
Subject:
Physical Therapy
Received: 7/02/2023 | Accepted: 25/07/2023 | Published: 1/01/2024
Received: 7/02/2023 | Accepted: 25/07/2023 | Published: 1/01/2024
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
