

Volume 24, Issue 2 (Summer 2023)
jrehab 2023, 24(2): 264-283 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khoddami S M, Aghadoost S, Khatoonabadi A R, Dabirmoghaddam P, Jalaie S. Comparison and Relation Between Vocal Tract Discomfort and Voice Handicap Index in Teachers With and Without Muscle Tension Dysphonia. jrehab 2023; 24 (2) :264-283
URL: http://rehabilitationj.uswr.ac.ir/article-1-3164-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3164-en.html
Seyyedeh Maryam Khoddami1 

 , Samira Aghadoost * 2, Ahmad Reza Khatoonabadi1 , Payman Dabirmoghaddam3 , Shohreh Jalaie4
, Samira Aghadoost * 2, Ahmad Reza Khatoonabadi1 , Payman Dabirmoghaddam3 , Shohreh Jalaie4
, Samira Aghadoost * 2, Ahmad Reza Khatoonabadi1 , Payman Dabirmoghaddam3 , Shohreh Jalaie4
1- Department of Speech Therapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
2- Department of Speech Therapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran. , samira.aghadoost@gmail.com
3- Department of Ear, Nose and Throat (ENT), School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
4- Department of Physiotherapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
2- Department of Speech Therapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran. , samira.aghadoost@gmail.com
3- Department of Ear, Nose and Throat (ENT), School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
4- Department of Physiotherapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 2145 kb]
(525 Downloads)
| Abstract (HTML) (2487 Views)
Full-Text: (920 Views)
Introduction
Professional voice users like teachers are more at risk of voice disorders than other voice users due to their special job conditions, such as speaking for a long time and usually in a crowded environment. Muscle tension dysphonia (MTD) is one of the common voice problems among teachers [2-5]. Various etiological factors have been identified as the cause of voice disorder in teachers, including conditions of the educational environment, lifestyle, various diseases, and bad and incorrect use of voice [10, 11, 12]. The main cause of voice complaints among teachers seems to be bad and incorrect use of voice in inappropriate audio conditions. This situation increases muscle tension in the larynx and its surrounding areas. In other words, teachers’ complaints during the day, especially at the end of the working day, indicate more muscle tension in the larynx and its surrounding areas, known as MTD in the literature [14, 15]. The term MTD, first presented in 1983 by Morrison et al., represents a type of voice functional disorder with a biomechanical view of muscle tension disorders caused by voice overwork [15]. MTD is diagnosed by confirming voice complaint, voice disorder, tension in larynx muscles during palpation examination, and breathing or vocalization during videosterboscopic examination [16].
Patients with voice disorders can be evaluated by different methods, such as auditory-perceptual evaluation of voice, acoustic, aerodynamic, larynx touch, self-perception questionnaires, and examination of the structure and function of the larynx. Self-perception questionnaires, such as vocal tract discomfort (VTD) and the voice handicap index (VHI) questionnaires, are used by patients to check their attitude toward voice disorder or to investigate audio-related complaints. Self-reporting can be employed to understand the clients’ unpleasant feelings after suffering from a voice disorder, the awareness level of voice problems, and the impact of hoarseness on their general and voice-related quality of life (QoL) [18].
Apart from increasing the teachers’ awareness about the occurrence of voice disorders in the future, it is possible to provide preventive measures and to determine the specialized clinical measures needed for audiotherapists and otolaryngologists using these two voice self-assessments. Considering that both questionnaires are self-perception and the complaints of patients’ voices are extracted from different dimensions, it is assumed that the scores of these questionnaires are affected by and related to each other. This study was conducted to compare the results of VTD in primary school teachers with and without MTD and examine the correlation of two self-assessment questionnaires of voice disorders, i.e., VTD and VHI, between two groups of teachers with and without MTD.
Materials and Methods
The research method was descriptive-analytical, non-interventional, and cross-sectional. The study participants included 80 female primary school teachers who entered the study in two separate groups. The first group included 40 teachers with MTD with an average age of 39.44 ±6.37 years. The second group included 40 teachers with an average age of 40.63±5.17 years, who had normal voices based on expert evaluations and did not receive an MTD diagnosis.
The participants were selected among the female public primary school education teachers in Tehran City, Iran. First, by convenience sampling, 15 girls’ public primary schools were chosen from education districts 5 and 2 of Tehran City.
After examining the general conditions for entering the study based on the personal profile form and voice history, the teachers with a voice problem were invited for further research. Then, based on the voice history, according to their report, and the result of the informal auditory-perceptual evaluation of the voice performed by the speech therapist, dysphonia was confirmed in them. Afterward, an experienced speech therapist performed more specialized assessments, including palpation of the larynx and observation of the larynx to evaluate and treat voice disorders. After selecting the teachers with MTD, the teachers of the second group were selected. To select the group’s teachers without MTD, they should have no voice complaints and the general conditions of entering the study.
After selecting qualified teachers and grouping them into groups with and without MTD, the discomfort experienced in the vocal tract was evaluated through the Persian version of the VTD scale and the level of perceived voice disability using the VHI. Both scales are valid and reliable for investigating self-perception of acoustic problems in Persian [28, 32].
The study results are part of the PhD thesis in speech therapy at the Tehran University of Medical Sciences. Ethical approval was obtained from the Ethics Committee of Tehran University of Medical Sciences under the number IR TUMS.VCR.REC.1396.4091 to conduct the study. Before the implementation of the study, the participants expressed their consent to participate in the study in the form of an informed consent form. The obtained data were analyzed using SPSS software, version 20. Before analyzing the data and selecting the appropriate test to compare the results between the two groups of participants, the distribution of the VTD and VHI scale scores was investigated using the Kolmogorov-Smirnov test. In the present study, a significance level of 0.05 was considered.
Results
The research subjects were 80 female teachers in the first to sixth grades of public girls’ schools in Tehran, aged 25 to 45 years. Table 1 presents the demographic characteristics of the participating teachers in the two groups separately.
Comparing the two groups, no significant difference was observed regarding the average characteristics of age (P=0.42), teaching experience (P=0.39), and teaching hours (P=0.44).
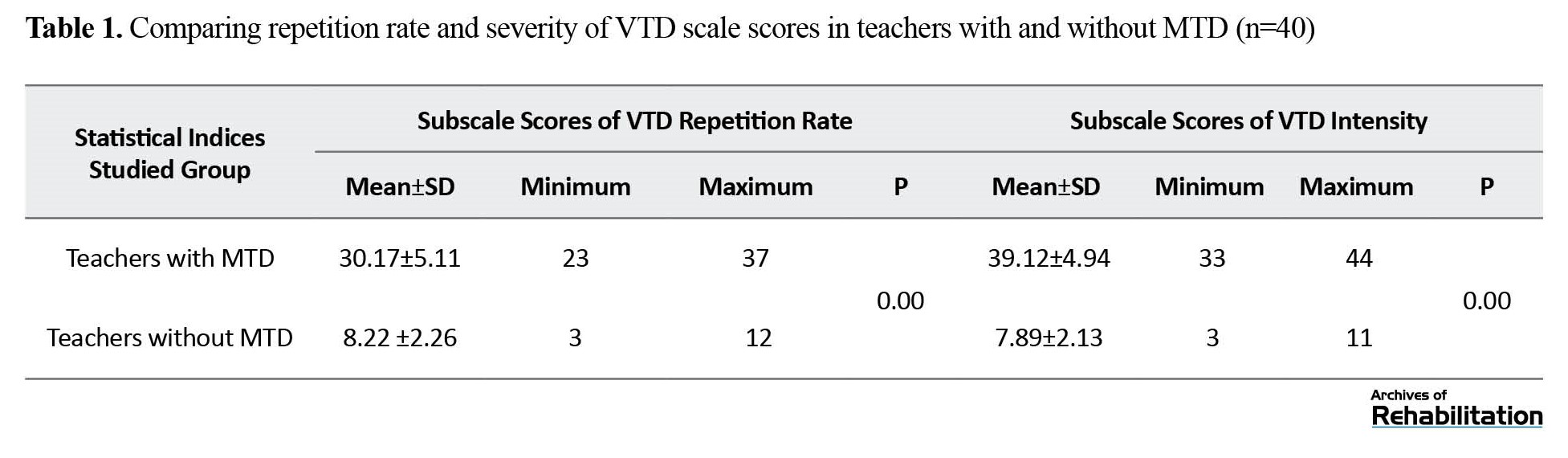
Table 1 presents the descriptive and analytical results of completing the VTD scale, separated by the two subscales of the repetition rate and the intensity of discomfort in teachers with and without MTD using the independent t test.
Table 1 presents that the average score of the repetition rate subscale of the VTD scale in the group of teachers with MTD is much higher than teachers without MTD. The result of the independent t test also showed that this difference was statistically significant between the two groups of teachers (P<0.05). Also, the analysis of the results using the independent t test showed that the mean score of the severity subscale of the VTD scale in teachers with MTD was significantly higher than that reported in the group of teachers without MTD (P<0.05).
Also, Table 2 presents the analysis of the VHI questionnaire separately in four parts of the total score, physical subtest, emotional subtest, and performance subtest in teachers with and without MTD using the independent t test.
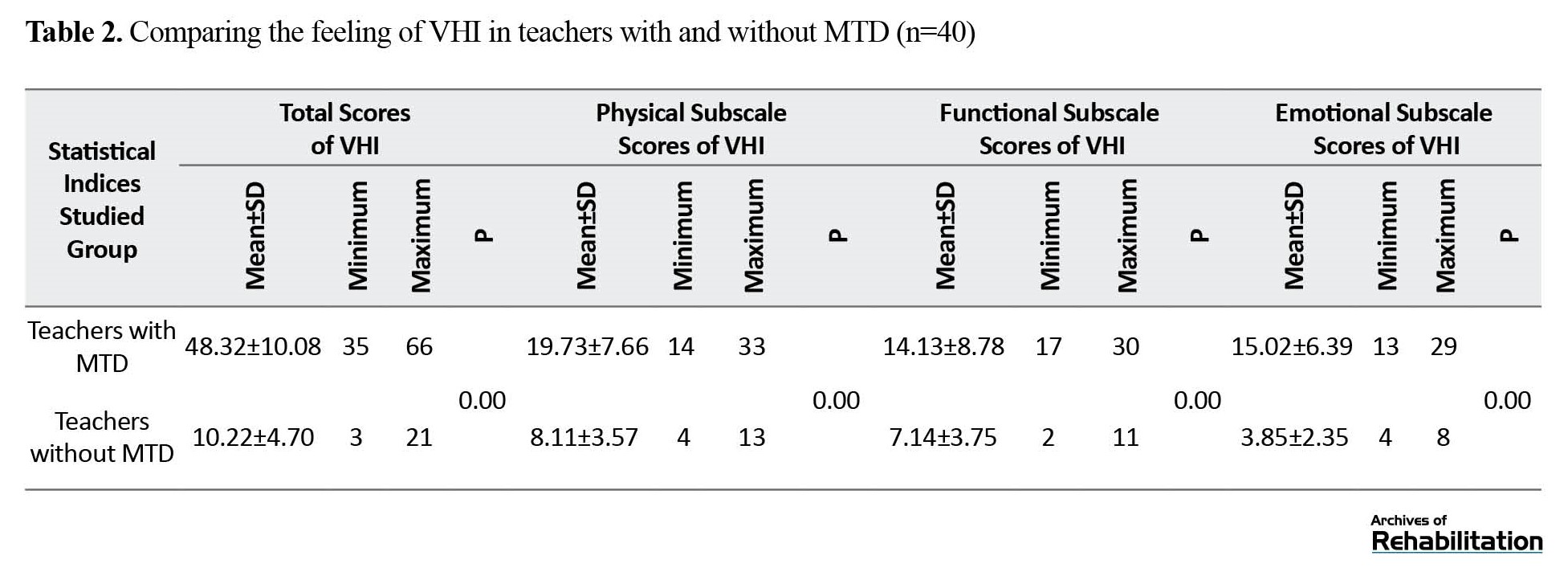
As seen in Table 2, the average total score (63.82 vs 10.22) and VHI subtests in teachers with MTD is higher than in teachers without MTD, and this difference is statistically significant (P<0.05).
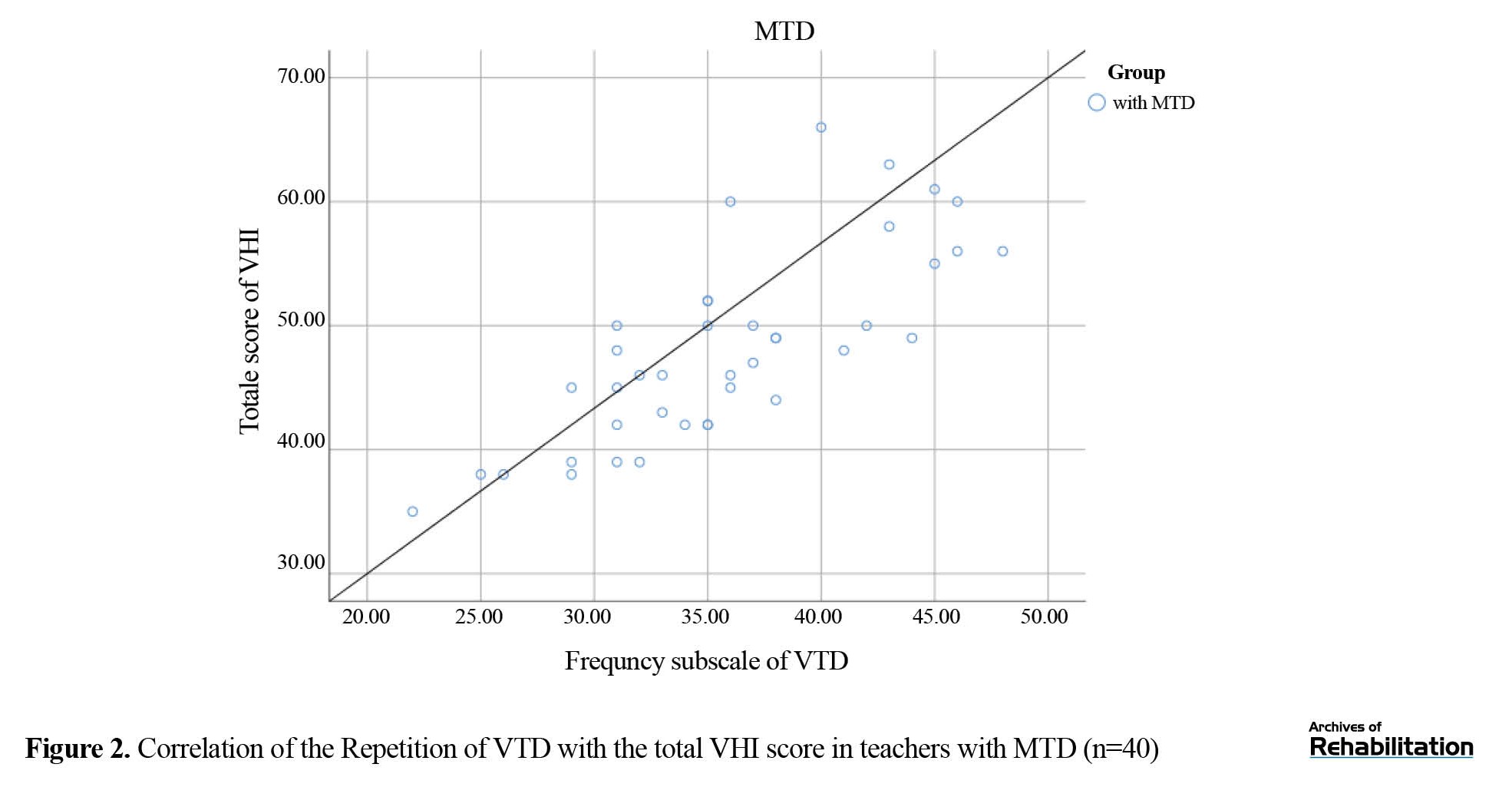
Also, the correlation analysis using the Pearson test showed a significant positive relationship between the VHI total score and the two subscales of repetition rate and severity of VTD discomfort in teachers with MTD (r:0.92 and r:0.91, respectively). This relationship was also significant in teachers without MTD (r:0.39 and r: 0.43, respectively). Figure 1 shows the relationship between the VTD severity subtest and the total VHI score.
 Figure 2 shows the relationship between the VTD repetition subtest and the total VHI score in teachers with MTD.
Figure 2 shows the relationship between the VTD repetition subtest and the total VHI score in teachers with MTD.
 Discussion
Discussion
The present study was conducted to investigate and compare the results of two voice self-perception questionnaires (the VTD and VHI questionnaires) and to determine their correlation in teachers with and without MTD. The results showed that teachers with MTD scored higher in the subscales of repetition and severity of VTD and in the total score and subscales of VHI compared to teachers without MTD. According to the noticeable difference between the two groups, this finding indicates more intensity of discomfort that female teachers with MTD felt in their vocal tract. In addition, the results of the present study showed that teachers with MTD obtained higher scores in all parts of the VHI questionnaire, which indicates a higher voice disability and a lower voice-related quality of life. Teachers without MTD also experience some unpleasant sensations in their vocal tract and vocal disability related to their specific job conditions.
The VTD scale has been used for various research objectives. Some studies conducted in this field have examined the VTD scale in teachers and have not compared it between different groups. For example, Galletti et al. investigated the power of VTD to predict and identify future voice problems of teachers. Their study’s results also indicated this scale’s ability to identify teachers at risk for voice problems in the future [22]. Some foreign studies conducted on teachers have compared the results of this scale in different groups of teachers. Rodrigues et al. examined the relationship between voice self-perception and VTD symptoms in teachers with voice complaints. Their research confirmed the relationship between the two variables and reported that teachers with voice complaints have a higher repetition and intensity of VTD than teachers without voice complaints. Therefore, the researchers noted that the VTD scale could be a predictive tool for primary voice disorder [21]. The results of these previous studies show that teachers, as one of the groups of professional audio users, are at risk of various unpleasant sensory experiences in the vocal tract, and various factors, such as the presence or absence of voice complaints as well as their teaching conditions can affect repetition and intensity of these unpleasant sensory experiences. However, it was expected that teachers with MTD would score high on the self-perception scale of VTD compared to teachers without MTD. Considering that no significant difference was observed between the two investigated groups in terms of the number of students, teaching experience, age, and duration of teaching, it seems that the significance of the difference in VTD results between the two groups of teachers is due to the presence of MTD.
As mentioned before, the VHI self-perception questionnaire is among voice-related quality-of-life assessment tools, which includes emotional, physical, and social dimensions related to voice and measures the degree of disability due to voice disorder. Since disability means the presence of limitations in performing daily social activities due to impairment and disability, voice disorder can increase the feeling of voice disability and reduce the quality of life. In teachers with MTD, the results of this questionnaire were significantly higher than in teachers without MTD, which indicates self-perception of the psychosocial consequences of voice disorders. Previous studies showed increased muscle tension leads to significant disability and functional limitations in MTD patients. It seems that the lack of knowledge of teachers about the impact of using incorrect vocalization behaviors, physical pressure on the larynx, mental pressure on the quality of their voice, and the inability to control their mental states and manage their stress has led to an increased score of this questionnaire and its subtests in teachers with MTD. Various studies have been conducted to examine VHI in teachers with MTD, all of which have pointed out the high VHI score in teachers with MTD, and their results were consistent with the present study [29, 31, 36]. Aghadost et al. compared the VHI score between teachers with and without MTD. They mentioned that teachers with MTD felt more vocal disability than teachers without MTD, consistent with the present study’s findings [30].
Conclusion
Finally, the results of the present study showed that in some cases, even symptoms of voice hoarseness and voice fatigue exist in teachers, but these symptoms may be ignored due to their repetitiveness. However, the information extracted from self-perception questionnaires, such as VTD and VHI, can effectively identify patients’ complaints and plan appropriate treatment plans in the future. In addition to helping identify voice complaints and unpleasant feelings of the vocal tract in teachers with voice problems and MTD, they can also be useful and efficient in predicting the occurrence of voice problems and the need for more detailed evaluations in teachers without MTD. In future studies, it is suggested to investigate the correlation of this self-perception tool by the patient with other stroboscopic, perceptual, and acoustic evaluations to investigate the relationship between different aspects of voice in teachers with MTD to start early intervention to take care of voice and larynx, if necessary, relying on more accessible evaluation. It is also suggested to conduct more studies in this field among professional voice users to understand the importance of the predictive power of these available and quick questionnaires as a screening tool. Considering that one of the limitations of the present study was examining the results of VTD and VHI only in female teachers, further studies on both groups of male and female teachers and examining the possible factor of gender on self-perception results are also recommended.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tehran University of Medical Sciences (Code: IR.TUMS.VCR.REC.1396.4091). Before the study, the participants signed an informed consent form.
Funding
The paper was extracted from the PhD thesis of Samira Aghadoost, approved by the Department of Speech Therapy, School of Rehabilitation, Tehran University of Medical Sciences. This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision, data analysis, review & editing: Seyyedeh Maryam Khoddami; Methodology, data analysis, and original draft preparation: Samira Aghadoost; Conceptualization: Ahmad Reza Khatoonabadi; methodology: Payman Dabirmoghaddam; Statistical analysis: Shohreh Jalaie.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all the teachers participated in this study for their cooperation.
References
Professional voice users like teachers are more at risk of voice disorders than other voice users due to their special job conditions, such as speaking for a long time and usually in a crowded environment. Muscle tension dysphonia (MTD) is one of the common voice problems among teachers [2-5]. Various etiological factors have been identified as the cause of voice disorder in teachers, including conditions of the educational environment, lifestyle, various diseases, and bad and incorrect use of voice [10, 11, 12]. The main cause of voice complaints among teachers seems to be bad and incorrect use of voice in inappropriate audio conditions. This situation increases muscle tension in the larynx and its surrounding areas. In other words, teachers’ complaints during the day, especially at the end of the working day, indicate more muscle tension in the larynx and its surrounding areas, known as MTD in the literature [14, 15]. The term MTD, first presented in 1983 by Morrison et al., represents a type of voice functional disorder with a biomechanical view of muscle tension disorders caused by voice overwork [15]. MTD is diagnosed by confirming voice complaint, voice disorder, tension in larynx muscles during palpation examination, and breathing or vocalization during videosterboscopic examination [16].
Patients with voice disorders can be evaluated by different methods, such as auditory-perceptual evaluation of voice, acoustic, aerodynamic, larynx touch, self-perception questionnaires, and examination of the structure and function of the larynx. Self-perception questionnaires, such as vocal tract discomfort (VTD) and the voice handicap index (VHI) questionnaires, are used by patients to check their attitude toward voice disorder or to investigate audio-related complaints. Self-reporting can be employed to understand the clients’ unpleasant feelings after suffering from a voice disorder, the awareness level of voice problems, and the impact of hoarseness on their general and voice-related quality of life (QoL) [18].
Apart from increasing the teachers’ awareness about the occurrence of voice disorders in the future, it is possible to provide preventive measures and to determine the specialized clinical measures needed for audiotherapists and otolaryngologists using these two voice self-assessments. Considering that both questionnaires are self-perception and the complaints of patients’ voices are extracted from different dimensions, it is assumed that the scores of these questionnaires are affected by and related to each other. This study was conducted to compare the results of VTD in primary school teachers with and without MTD and examine the correlation of two self-assessment questionnaires of voice disorders, i.e., VTD and VHI, between two groups of teachers with and without MTD.
Materials and Methods
The research method was descriptive-analytical, non-interventional, and cross-sectional. The study participants included 80 female primary school teachers who entered the study in two separate groups. The first group included 40 teachers with MTD with an average age of 39.44 ±6.37 years. The second group included 40 teachers with an average age of 40.63±5.17 years, who had normal voices based on expert evaluations and did not receive an MTD diagnosis.
The participants were selected among the female public primary school education teachers in Tehran City, Iran. First, by convenience sampling, 15 girls’ public primary schools were chosen from education districts 5 and 2 of Tehran City.
After examining the general conditions for entering the study based on the personal profile form and voice history, the teachers with a voice problem were invited for further research. Then, based on the voice history, according to their report, and the result of the informal auditory-perceptual evaluation of the voice performed by the speech therapist, dysphonia was confirmed in them. Afterward, an experienced speech therapist performed more specialized assessments, including palpation of the larynx and observation of the larynx to evaluate and treat voice disorders. After selecting the teachers with MTD, the teachers of the second group were selected. To select the group’s teachers without MTD, they should have no voice complaints and the general conditions of entering the study.
After selecting qualified teachers and grouping them into groups with and without MTD, the discomfort experienced in the vocal tract was evaluated through the Persian version of the VTD scale and the level of perceived voice disability using the VHI. Both scales are valid and reliable for investigating self-perception of acoustic problems in Persian [28, 32].
The study results are part of the PhD thesis in speech therapy at the Tehran University of Medical Sciences. Ethical approval was obtained from the Ethics Committee of Tehran University of Medical Sciences under the number IR TUMS.VCR.REC.1396.4091 to conduct the study. Before the implementation of the study, the participants expressed their consent to participate in the study in the form of an informed consent form. The obtained data were analyzed using SPSS software, version 20. Before analyzing the data and selecting the appropriate test to compare the results between the two groups of participants, the distribution of the VTD and VHI scale scores was investigated using the Kolmogorov-Smirnov test. In the present study, a significance level of 0.05 was considered.
Results
The research subjects were 80 female teachers in the first to sixth grades of public girls’ schools in Tehran, aged 25 to 45 years. Table 1 presents the demographic characteristics of the participating teachers in the two groups separately.
Comparing the two groups, no significant difference was observed regarding the average characteristics of age (P=0.42), teaching experience (P=0.39), and teaching hours (P=0.44).
Table 1 presents the descriptive and analytical results of completing the VTD scale, separated by the two subscales of the repetition rate and the intensity of discomfort in teachers with and without MTD using the independent t test.
Table 1 presents that the average score of the repetition rate subscale of the VTD scale in the group of teachers with MTD is much higher than teachers without MTD. The result of the independent t test also showed that this difference was statistically significant between the two groups of teachers (P<0.05). Also, the analysis of the results using the independent t test showed that the mean score of the severity subscale of the VTD scale in teachers with MTD was significantly higher than that reported in the group of teachers without MTD (P<0.05).
Also, Table 2 presents the analysis of the VHI questionnaire separately in four parts of the total score, physical subtest, emotional subtest, and performance subtest in teachers with and without MTD using the independent t test.
As seen in Table 2, the average total score (63.82 vs 10.22) and VHI subtests in teachers with MTD is higher than in teachers without MTD, and this difference is statistically significant (P<0.05).
Also, the correlation analysis using the Pearson test showed a significant positive relationship between the VHI total score and the two subscales of repetition rate and severity of VTD discomfort in teachers with MTD (r:0.92 and r:0.91, respectively). This relationship was also significant in teachers without MTD (r:0.39 and r: 0.43, respectively). Figure 1 shows the relationship between the VTD severity subtest and the total VHI score.
The present study was conducted to investigate and compare the results of two voice self-perception questionnaires (the VTD and VHI questionnaires) and to determine their correlation in teachers with and without MTD. The results showed that teachers with MTD scored higher in the subscales of repetition and severity of VTD and in the total score and subscales of VHI compared to teachers without MTD. According to the noticeable difference between the two groups, this finding indicates more intensity of discomfort that female teachers with MTD felt in their vocal tract. In addition, the results of the present study showed that teachers with MTD obtained higher scores in all parts of the VHI questionnaire, which indicates a higher voice disability and a lower voice-related quality of life. Teachers without MTD also experience some unpleasant sensations in their vocal tract and vocal disability related to their specific job conditions.
The VTD scale has been used for various research objectives. Some studies conducted in this field have examined the VTD scale in teachers and have not compared it between different groups. For example, Galletti et al. investigated the power of VTD to predict and identify future voice problems of teachers. Their study’s results also indicated this scale’s ability to identify teachers at risk for voice problems in the future [22]. Some foreign studies conducted on teachers have compared the results of this scale in different groups of teachers. Rodrigues et al. examined the relationship between voice self-perception and VTD symptoms in teachers with voice complaints. Their research confirmed the relationship between the two variables and reported that teachers with voice complaints have a higher repetition and intensity of VTD than teachers without voice complaints. Therefore, the researchers noted that the VTD scale could be a predictive tool for primary voice disorder [21]. The results of these previous studies show that teachers, as one of the groups of professional audio users, are at risk of various unpleasant sensory experiences in the vocal tract, and various factors, such as the presence or absence of voice complaints as well as their teaching conditions can affect repetition and intensity of these unpleasant sensory experiences. However, it was expected that teachers with MTD would score high on the self-perception scale of VTD compared to teachers without MTD. Considering that no significant difference was observed between the two investigated groups in terms of the number of students, teaching experience, age, and duration of teaching, it seems that the significance of the difference in VTD results between the two groups of teachers is due to the presence of MTD.
As mentioned before, the VHI self-perception questionnaire is among voice-related quality-of-life assessment tools, which includes emotional, physical, and social dimensions related to voice and measures the degree of disability due to voice disorder. Since disability means the presence of limitations in performing daily social activities due to impairment and disability, voice disorder can increase the feeling of voice disability and reduce the quality of life. In teachers with MTD, the results of this questionnaire were significantly higher than in teachers without MTD, which indicates self-perception of the psychosocial consequences of voice disorders. Previous studies showed increased muscle tension leads to significant disability and functional limitations in MTD patients. It seems that the lack of knowledge of teachers about the impact of using incorrect vocalization behaviors, physical pressure on the larynx, mental pressure on the quality of their voice, and the inability to control their mental states and manage their stress has led to an increased score of this questionnaire and its subtests in teachers with MTD. Various studies have been conducted to examine VHI in teachers with MTD, all of which have pointed out the high VHI score in teachers with MTD, and their results were consistent with the present study [29, 31, 36]. Aghadost et al. compared the VHI score between teachers with and without MTD. They mentioned that teachers with MTD felt more vocal disability than teachers without MTD, consistent with the present study’s findings [30].
Conclusion
Finally, the results of the present study showed that in some cases, even symptoms of voice hoarseness and voice fatigue exist in teachers, but these symptoms may be ignored due to their repetitiveness. However, the information extracted from self-perception questionnaires, such as VTD and VHI, can effectively identify patients’ complaints and plan appropriate treatment plans in the future. In addition to helping identify voice complaints and unpleasant feelings of the vocal tract in teachers with voice problems and MTD, they can also be useful and efficient in predicting the occurrence of voice problems and the need for more detailed evaluations in teachers without MTD. In future studies, it is suggested to investigate the correlation of this self-perception tool by the patient with other stroboscopic, perceptual, and acoustic evaluations to investigate the relationship between different aspects of voice in teachers with MTD to start early intervention to take care of voice and larynx, if necessary, relying on more accessible evaluation. It is also suggested to conduct more studies in this field among professional voice users to understand the importance of the predictive power of these available and quick questionnaires as a screening tool. Considering that one of the limitations of the present study was examining the results of VTD and VHI only in female teachers, further studies on both groups of male and female teachers and examining the possible factor of gender on self-perception results are also recommended.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tehran University of Medical Sciences (Code: IR.TUMS.VCR.REC.1396.4091). Before the study, the participants signed an informed consent form.
Funding
The paper was extracted from the PhD thesis of Samira Aghadoost, approved by the Department of Speech Therapy, School of Rehabilitation, Tehran University of Medical Sciences. This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision, data analysis, review & editing: Seyyedeh Maryam Khoddami; Methodology, data analysis, and original draft preparation: Samira Aghadoost; Conceptualization: Ahmad Reza Khatoonabadi; methodology: Payman Dabirmoghaddam; Statistical analysis: Shohreh Jalaie.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all the teachers participated in this study for their cooperation.
References
- Murry T, Rosen CA. Vocal education for the professional voice user and singer. Otolaryngologic Clinics of North America. 2000; 33(5):967-81. [DOI:10.1016/S0030-6665(05)70258-9] [PMID]
- Martins RH, Pereira ER, Hidalgo CB, Tavares EL. Voice disorders in teachers. A review. Journal of Voice. 2014; 28(6):716-24. [DOI:10.1016/j.jvoice.2014.02.008] [PMID]
- Cardoso JP, Araújo TM, Carvalho FM, Oliveira NF, Reis EJ. [Psychosocial work-related factors and musculoskeletal pain among schoolteachers (Portuguese)]. Cadernos de Saude Publica. 2011; 27(8):1498-506. [DOI:10.1590/S0102-311X2011000800005] [PMID]
- Aghadoost S, Jalaie S, Khatoonabadi AR, Dabirmoghaddam P, Khoddami SM. A study of vocal facilitating techniques compared to manual circumlaryngeal therapy in teachers with muscle tension dysphonia. Journal of Voice. 2020; 34(6):963.e11-963.e21. [DOI:10.1016/j.jvoice.2019.06.002] [PMID]
- Roy N, Merrill RM, Thibeault S, Parsa RA, Gray SD, Smith EM. Prevalence of voice disorders in teachers and the general population. Journal of Speech, Language, and Hearing Research. 2004; 47(2):281-93. [DOI:10.1044/1092-4388(2004/023)] [PMID]
- Munier C, Kinsella R. The prevalence and impact of voice problems in primary school teachers. Occupational Medicine. 2008; 58(1):74-6. [DOI:10.1093/occmed/kqm104] [PMID]
- Smith E, Gray SD, Dove H, Kirchner L, Heras H. Frequency and effects of teachers’ voice problems. Journal of Voice. 1997; 11(1):81-7. [DOI:10.1016/S0892-1997(97)80027-6] [PMID]
- Russell A, Oates J, Greenwood KM. Prevalence of voice problems in teachers. Journal of Voice. 1998; 12(4):467-79. [DOI:10.1016/S0892-1997(98)80056-8] [PMID]
- Aghadoost O, Amiri-Shavaki Y, Moradi N, Jalai S. A comparison of dysphonia severity index in female teachers with and without voice complaints in elementary schools of Tehran, Iran. Nursing and Midwifery Studies. 2013; 1(3):133-8. [Link]
- Kooijman PG, de Jong FI, Thomas G, Huinck W, Donders R, Graamans K, et al. Risk factors for voice problems in teachers. Folia Phoniatrica et Logopaedica. 2006; 58(3):159-74. [DOI:10.1159/000091730] [PMID]
- Chen SH, Chiang SC, Chung YM, Hsiao LC, Hsiao TY. Risk factors and effects of voice problems for teachers. Journal of Voice. 2010; 24(2):183-92. [DOI:10.1016/j.jvoice.2008.07.008] [PMID]
- Miller MK, Verdolini K. Frequency and risk factors for voice problems in teachers of singing and control subjects. Journal of Voice. 1995; 9(4):348-62. [DOI:10.1016/S0892-1997(05)80197-3] [PMID]
- Nguyen DD, Kenny DT. Randomized controlled trial of vocal function exercises on muscle tension dysphonia in Vietnamese female teachers. Journal of Otolaryngology--Head & Neck Surgery. 2009; 38(2):261-78. [PMID]
- Mathieson L, Hirani SP, Epstein R, Baken RJ, Wood G, Rubin JS. Laryngeal manual therapy: A preliminary study to examine its treatment effects in the management of muscle tension dysphonia. Journal of Voice. 2009; 23(3):353-66. [DOI:10.1016/j.jvoice.2007.10.002] [PMID]
- Morrison MD, Rammage LA, Belisle GM, Pullan CB, Nichol H. Muscular tension dysphonia. The Journal of Otolaryngology. 1983; 12(5):302-6. [PMID]
- Khoddami SM, Nakhostin Ansari N, Izadi F, Talebian Moghadam S. The assessment methods of laryngeal muscle activity in muscle tension dysphonia: A review. The Scientific World Journal. 2013; 2013:507397. [DOI:10.1155/2013/507397] [PMID] [PMCID]
- Moradi N, Maroufi N, Bijankhan M, Hosseinzadeh Nik T, Salavati M, Jalayer T, et al. Intrarater and interrater reliability of sagittal head posture: A novel technique performed by a physiotherapist and a speech and language pathologist. Journal of Voice. 2014; 28(6):842.e11-6. [DOI:10.1016/j.jvoice.2014.02.014] [PMID]
- Lopes LW, de Oliveira Florencio V, Silva POC, da Nóbrega E Ugulino AC, Almeida AA. Vocal Tract Discomfort Scale (VTDS) and Voice Symptom Scale (VoiSS) in the evaluation of patients with voice disorders. Journal of Voice. 2019; 33(3):381.e23-381.e32. [DOI:10.1016/j.jvoice.2017.11.018] [PMID]
- Jacobson BH, Johnson A, Grywalski C, Silbergleit A, Jacobson G, Benninger MS, et al. The voice handicap index (VHI): Development and validation. American Journal of Speech-Language Pathology. 1997; 6(3):66-70. [DOI:10.1044/1058-0360.0603.66]
- Amaral AC, Zambon F, Moreti F, Behlau M. Vocal tract discomfort in teachers after teaching activity. Codas. 2017; 29(2):e20160045. [PMID]
- Rodrigues G, Zambon F, Mathieson L, Behlau M. Vocal tract discomfort in teachers: Its relationship to self-reported voice disorders. Journal of Voice. 2013; 27(4):473-80. [DOI:10.1016/j.jvoice.2013.01.005] [PMID]
- Galletti B, Sireci F, Mollica R, Iacona E, Freni F, Martines F, et al. Vocal Tract Discomfort Scale (VTDS) and Voice Symptom Scale (VoiSS) in the early identification of Italian teachers with voice disorders. International Archives of Otorhinolaryngology. 2020; 24(3):e323-9. [DOI:10.1055/s-0039-1700586] [PMID] [PMCID]
- Korn GP, Augusto de Lima Pontes A, Abranches D, Augusto de Lima Pontes P. Vocal tract discomfort and risk factors in university teachers. Journal of Voice. 2016; 30(4):507.e1-8. [DOI:10.1016/j.jvoice.2015.06.001] [PMID]
- Tahamtan M, Kakavandi A, Scherer RC, Vahedi M. Vocal tract discomfort symptoms in elementary and high school teachers. Journal of Voice. 2023; 37(1):68-78. [PMID]
- Mendes AL, Lucena BT, De Araújo AM, Melo LP, Lopes LW, Silva MF. Teacher’s voice: Vocal tract discomfort symptoms, vocal intensity and noise in the classroom. Codas. 2016; 28(2):168-75. [DOI:10.1590/2317-1782/20162015027] [PMID]
- Khoramshahi H, Dehqan A, Scherer RC, Sharifi Z, Ahmadi S. Comparison of vocal fatigue and vocal tract discomfort between teachers of normal pupils and teachers of mentally disabled pupils. European Archives of Oto-Rhino-Laryngology. 2021; 278(7):2429-36. [DOI:10.1007/s00405-021-06863-w] [PMID]
- Sabzevari F, Shavaki Y, Kamali M. [Correlation between vocal tract discomfort and quality of life in female elementary-school teachers of Tehran (Persian)]. Middle Eastern Journal of Disability Studies. 2017; 7:70. [Link]
- Torabi H, Khoddami SM, Ansari NN, Dabirmoghaddam P. The Vocal Tract Discomfort Scale: Validity and reliability of the Persian version in the assessment of patients with muscle tension dysphonia. Journal of Voice. 2016; 30(6):711-6. [DOI:10.1016/j.jvoice.2015.08.002] [PMID]
- Niebudek-Bogusz E, Woznicka E, Zamyslowska-Szmytke E, Sliwinska-Kowalska M. Correlation between acoustic parameters and Voice Handicap Index in dysphonic teachers. Folia Phoniatrica et Logopaedica. 2010; 62(1-2):55-60. [DOI:10.1159/000239064] [PMID]
- Aghadoost S, Jalaie S, Dabirmoghaddam P, Khoddami SM. Effect of muscle tension dysphonia on self-perceived voice handicap and multiparametric measurement and their relation in female teachers. Journal of Voice. 2022; 36(1):68-75. [DOI:10.1016/j.jvoice.2020.04.011] [PMID]
- da Rocha LM, de Mattos Souza LD. Voice Handicap Index associated with common mental disorders in elementary school teachers. Journal of Voice. 2013; 27(5):595-602. [DOI:10.1016/j.jvoice.2012.10.001] [PMID]
- Moradi N, Pourshahbaz A, Soltani M, Javadipour S. Cutoff point at voice handicap index used to screen voice disorders among Persian speakers. Journal of Voice. 2013; 27(1):130.e1-. e5. [DOI:10.1016/j.jvoice.2012.08.007] [PMID]
- Moradi N, Pourshahbaz A, Soltani M, Javadipour S, Hashemi H, Soltaninejad N. Cross-cultural equivalence and evaluation of psychometric properties of voice handicap index into Persian. Journal of Voice. 2013; 27(2):258.e15-258.e22. [DOI:10.1016/j.jvoice.2012.09.006] [PMID]
- Van Houtte E, Van Lierde K, Claeys S. Pathophysiology and treatment of muscle tension dysphonia: A review of the current knowledge. Journal of Voice. 2011; 25(2):202-7. [DOI:10.1016/j.jvoice.2009.10.009] [PMID]
- Woźnicka E, Niebudek-Bogusz E, Kwiecień J, Wiktorowicz J, Śliwińska-Kowalska M. Applicability of the vocal tract discomfort (VTD) scale in evaluating the effects of voice therapy of occupational voice disorders. Medycyna Pracy. 2012; 63(2):141-52. [PMID]
- Kooijman PG, de Jong FI, Oudes MJ, Huinck W, van Acht H, Graamans K. Muscular tension and body posture in relation to voice handicap and voice quality in teachers with persistent voice complaints. Folia Phoniatrica et Logopaedica. 2005; 57(3):134-47. [DOI:10.1159/000084134] [PMID]
- Woźnicka E, Niebudek-Bogusz E, Wiktorowicz J, Sliwińska-Kowalska M. [Comparison of vocal tract discomfort scale results with objective and instrumental phoniatric parameters among teacher rehabilitees from voice disorders (Polish)]. Medycyna Pracy. 2013; 64(2):199-206. [PMID]
- Saeedi M, Yadegari M, Aghadoost S, Naderi M. Vocal tract discomfort and voice handicap index in patients undergoing thyroidectomy. Logopedics Phoniatrics Vocology. 2022; 47(1):49-55. [DOI:10.1080/14015439.2020.1864466] [PMID]
- Seifpanahi MS, Bayat B, Ghorbani Gholiabad S, Rezayi M. Self-rated vocal complaints relationship to Vocal Tract Discomfort and Singers Voice Handicap Index in Iranian religious singers. European Archives of Oto-Rhino-Laryngology. 2021; 278(7):2411-9. [PMID]
- Luyten A, Bruneel L, Meerschman I, D’haeseleer E, Behlau M, Coffé C, et al. Prevalence of vocal tract discomfort in the Flemish population without self-perceived voice disorders. Journal of Voice. 2016; 30(3):308-14. [DOI:10.1016/j.jvoice.2015.04.017] [PMID]
- Limoeiro FMH, Ferreira AEM, Zambon F, Behlau M. Comparison of the occurrence of signs and symptoms of vocal and change discomfort in the vocal tract in teachers from different levels of education. CoDAS. 2019; 31(2):e20180115. [PMID]
Type of Study: Original |
Subject:
Speech & Language Pathology
Received: 8/08/2022 | Accepted: 18/01/2023 | Published: 1/07/2023
Received: 8/08/2022 | Accepted: 18/01/2023 | Published: 1/07/2023
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Archives of Rehabilitation (RJ)
Journal Tel: +98 (21) 71732812, 09941095452 (Call time Saturday to Wednesday 8 to 14)
Publisher Tel: +9821 453 55 555 - 453 55 000
E-mail: rehabilitationjour@gmail.com
Archives of Rehabilitation (RJ)
Journal Tel: +98 (21) 71732812, 09941095452 (Call time Saturday to Wednesday 8 to 14)
Publisher Tel: +9821 453 55 555 - 453 55 000
E-mail: rehabilitationjour@gmail.com
