

Volume 23, Issue 4 (12-2022)
Arch Rehabil 2022, 23(4): 464-481 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohammadzadeh H, Zarezadeh A, Mardani M A, Sadeghi-Demneh E. Studying the Immediate Effects of Two Types of Thumb Splints on the Pain, Grip Strength, and Hand Function in People With De Quervain Tenosynovitis. Arch Rehabil 2022; 23 (4) :464-481
URL: http://rehabilitationj.uswr.ac.ir/article-1-3095-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3095-en.html

1- Department of Orthotics and Prosthetics, Student Research Committee, Faculty of Rehabilitation Sciences, Isfahan University of Medical Sciences, Isfahan, Iran., Faculty of Rehabilitation Sciences, Isfahan University of Medical Sciences, Hezar Jerib St., Isfahan, Iran
2- Department of Orthopaedic Surgery, Faculty of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran., : Faculty of Medicine, Isfahan University of Medical Sciences, Hezar Jerib St., Isfahan, Iran
3- Department of Orthotics and Prosthetics, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran., Department of Orthotics and Prosthetics, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
4- Department of Orthotics and Prosthetics, Musculoskeletal Research center, Faculty of Rehabilitation Sciences, Isfahan University of Medical Sciences, Isfahan, Iran. ,sadeghi@rehab.mui.ac.ir
2- Department of Orthopaedic Surgery, Faculty of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran., : Faculty of Medicine, Isfahan University of Medical Sciences, Hezar Jerib St., Isfahan, Iran
3- Department of Orthotics and Prosthetics, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran., Department of Orthotics and Prosthetics, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
4- Department of Orthotics and Prosthetics, Musculoskeletal Research center, Faculty of Rehabilitation Sciences, Isfahan University of Medical Sciences, Isfahan, Iran. ,
Full-Text [PDF 2147 kb]
(2419 Downloads)
| Abstract (HTML) (6051 Views)
Full-Text: (4916 Views)
Introduction
De Quervain tenosynovitis usually occurs due to inflammation and degenerative changes of the connective tissues in the first extensor compartment of the wrist [1, 2]. In this condition, the tendons of the abductor pollicis longus and extensor pollicis brevis muscles get stuck in the fibrous tunnel due to friction [1]. Although different opinions have been expressed regarding the type of tissue changes that can be the origin of de Quervain syndrome [3], there is a consensus regarding the presence of repetitive movements as the cause of tissue lesions. The onset of tendon involvement in the first extensor compartment of the wrist is accompanied by symptoms such as local pain and tenderness on the radial side of the wrist and the base of the thumb [4]. In people suffering from de Quervain tenosynovitis, holding objects in hand or ulnar deviation of the wrist causes stretching of the involved tissues and intensification of pain [1]. Accordingly, the power to grasp things is reduced, and slowness and inability in manual functions appear [5]. This disorder in manual function can also affect the daily activities of patients with this condition [6, 7].
To treat de Quervain tenosynovitis, non-surgical options are usually preferable [8]. According to scientific and clinical evidence, one of the conservative interventions commonly used for de Quervain tenosynovitis is to control the movements of the lesion site through a thumb splint [9]. Immobilization of the lesion site can be applied alone or with other conservative interventions, such as local injection [10]. For those suffering from de Quervain, a splint called a thumb spica is used, which, while placed on the forearm and wrist areas, surrounds the thumb and its middle joint [11]. The purpose of using the thumb spica splint is to limit the movements in the carpometacarpal and metacarpophalangeal joints of the first finger [12]. Therefore, wearing the thumb spica splint stabilizes the base joints of the thumb and creates a state of rest in the involved tendon [13, 14]. So, using a thumb spica splint is expected to effectively reduce inflammation and accelerate the healing of the lesion site [1, 13].
To treat de Quervain tenosynovitis, the proximal joints of the thumb are immobilized in the abduction position to prevent flexion of the thumb and stretching of the damaged tendons on the carpometacarpal and metacarpophalangeal joints of the first finger [5, 13, 14]. Considering that there are two abduction positions in the thumb (palmar [relatively vertical movement of the thumb away from the surface of the palm] and radial [movement of the thumb parallel to the surface of the palm or the radius bone]), it has not yet been determined which position can be more suitable for thumb spica splint design.
Based on what was discussed, the current study aimed to compare the effect of two types of splints with different positions of abduction (palmar and radial) of the thumb on pain, strength, and hand function in patients with de Quervain tenosynovitis.
Materials and Methods
This research was a quasi-experimental study. The samples were recruited by convenience non-probability sampling. The inclusion criteria included the presence of tenderness in the first extensor compartment of the wrist, the occurrence of pain (higher than score 3 based on the visual analog scale) in the radial part of the wrist, positive Finkelstein test, and extensor pollicis brevis tendon entrapment test [1, 5]. The exclusion criteria included corticosteroid injection in the wrist during the previous 3 months, surgery, fracture, severe osteoporosis, history of splint use, joint arthritis, or peripheral nerve involvement in the upper limb [15]. Also, there was no specific limit for the time of developing the complication, and people with acute and chronic lesions could enter the study. Before recruiting the samples and start the study, an ethical code was obtained, the volunteers were explained the study’s details and their written consent was obtained.
Thirty people with de Quervain tenosynovitis were evaluated in this study. Interventions included with and without splint palmar abduction and with splint radial thumb abduction. Splints kept the wrist at 15 degrees of extension (Figure 1). In the palmar abduction splint, the thumb was placed at 30 degrees of abduction and perpendicular to the palm (Figure 1A). In the radial abduction splint, the thumb was set at 30 degrees of abduction and parallel to the palm (Figure 1B). In splints, the interphalangeal joint of the thumb was outside the splint and moved freely.

The participants’ outcomes of pain intensity, grip strength, lateral pinch, palmar pinch strength, and manual function were measured in this study. The visual analog scale was used to measure pain intensity. People pressed a soft cylinder made of polyethylene foam in their palms. Then it was released, and the amount of pain during squeezing was marked on a 10 cm line. The number 0 means the absence of pain, and 10 means the most intense pain. The grip strength was measured through a hand dynamometer. The person pressed the dynamometer lever (SH5001, SAEHAN Inc., South Korea) with maximum power (Figure 2A) [16]. The pinch force was measured in both lateral and palmar pinches using a pinch gauge (SH5008, SAEHAN Inc., South Korea).
To measure the lateral pinch force, a person uses the pinch gauge as if he was holding a key and puts the maximum force into the movable button of the device with his thumb (Figure 2B). To record the palmar pinch force, the person holds the pinch dynamometer in the position of holding a needle between thumb and index fingers then applies a pinching force by the thumb (Figure 2C) [17]. The Jebsen-Taylor test was used to measure the manual performance of the participants. Jebsen test had seven subcategories (writing, turning over cards, picking up small objects, placing four beads on top of each other, moving light cans, moving heavy cans, and imitating movements while eating) [18]. A timer recorded the test execution time; recording a shorter time meant better manual performance.

The evaluations (except the Jebsen-Taylor evaluation) were repeated three times to reduce the error probability, and the average measurements were calculated and recorded. Statistical analysis was done using SPSS software, version 16. After confirming the normality of the data distribution by the Shapiro-Wilk test, the existence of differences in the study situations was checked by the analysis of variance (ANOVA) with repeated measures. In case of reporting a statistically significant difference between the study conditions, Bonferroni test was used for pairwise comparison of the intervention conditions. A significance level of 0.05 was considered in all tests.
Results
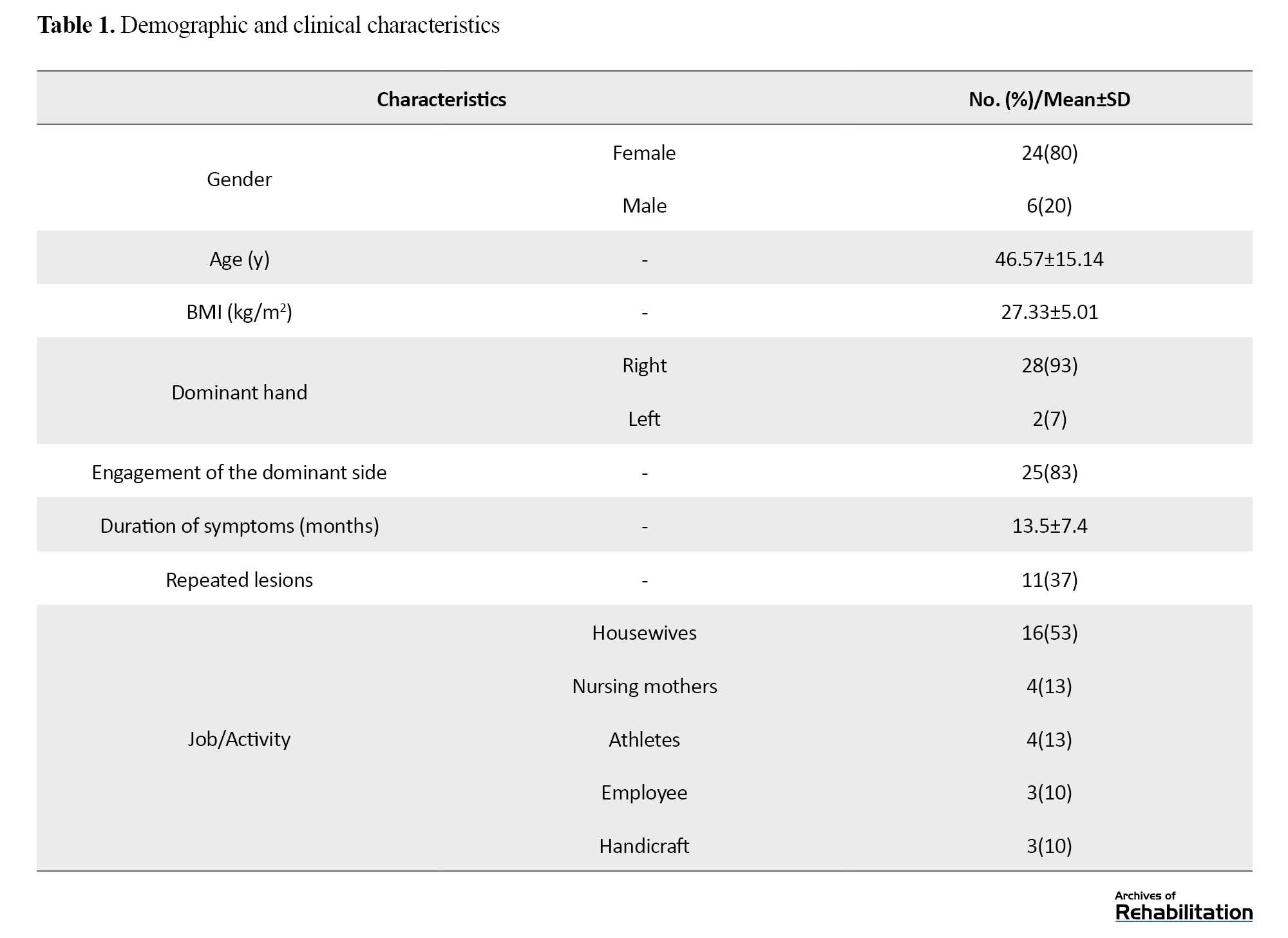
Descriptive statistics are presented in Table 1.
The results of the analysis of the variance test for repeated measures showed statistically significant differences between all study variables (Table 2).

To compare two by two study conditions, Bonferroni test was used in the output of variance analysis (Table 3), which showed that using both types of splints reduced pain.
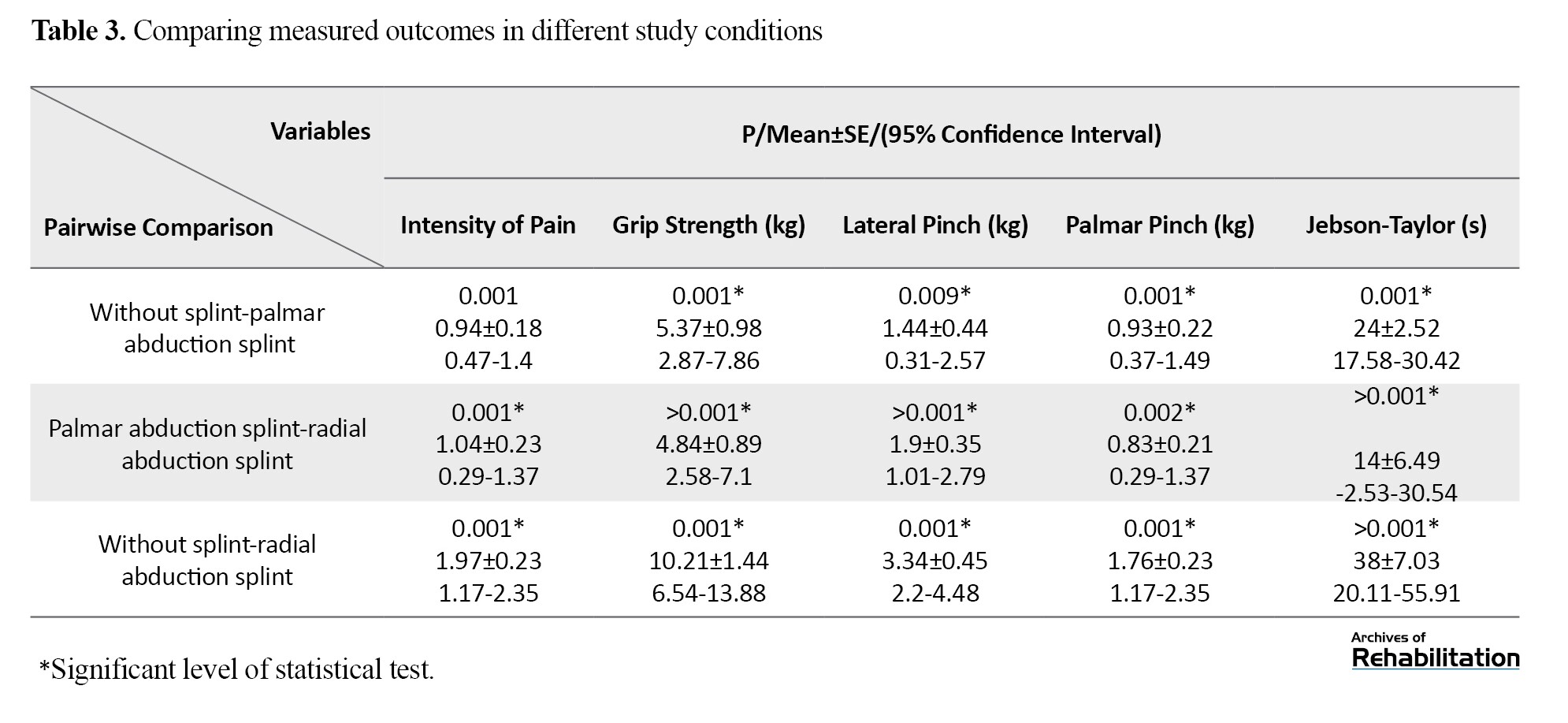
Using both types of splints has significantly reduced grip, lateral and palmar pinch strength and increased the time to perform the Jebsen-Taylor test. Comparing the two splints showed that the palmar abduction splint is more effective in reducing pain than the radial abduction splint. When using the palmar abduction splint, the grip, palmar pinch, and lateral pinch strength are greater than the radial abduction splint (P<0.001). However, no statistically significant difference was observed in comparing Jebsen test time between the two study splints (P=0.12).
Discussion
The use of plastic splints reduced the pain of de Quervain tenosynovitis. Since the splints limited the range of motion of the hand joints, they also reduced the function of the hand.
The use of thumb spica is one of the most common treatments for de Quervain tenosynovitis [13]. However, previous studies have reported the effectiveness of local injection more than thumb immobilization [19]. Some studies have also used immobilization methods such as bandages [20] and plastering [21]. Due to the definite ineffectiveness of local injection of corticosteroids in some cases, splints can be used as an alternative option or simultaneous with injection [22]. It is necessary to explain that splint treatment is not limited to conservative therapies and can also be used after surgery in patients with de Quervain tenosynovitis [23].
The wide range of applications of thumb splints in the treatment of tenosynovitis highlights the detection of the more effective types of this splint [5]. So far, what has been most important in the design of the thumb splint includes the restriction of wrist movements [24] and excessive movements [25], as well as, to some extent, compliance with the weight [26] and the duration of using the splint [27]. In the current study, in addition to controlling the lateral movements of the wrist, attention was also paid to the position of the thumb inside the splint. Paying attention to the carpometacarpal condition of the thumb in splints was the most important difference between this study and previous studies.
The results of this study showed that the use of splints reduces thumb spica while grasping objects. Reduction of pain following the use of a splint or thumb immobilization was also reported in all previous studies [9, 11, 20, 22, 28, 29]. To make it possible to investigate the immediate effect of the splints in this study, pain intensity was measured while pressing the foam cylinder in the palm to determine the role of the splint in reducing the momentary pressure on the lesion site. During the use of the palmar abduction splint, less pain was reported with the radial abduction splint. However, it cannot be interpreted as a direct result of a palmar abduction splint because the comfort of the position of the thumb inside the splint or the pressure of the edge of the splint on the thumb can also be involved in reporting the intensity of pain. It should also be noted that the report of pain can be influenced by the psychological and personality factors of people as well [30].
Previous studies show that palmar and lateral pinch force measurements are reduced as a reliable and valid variable in de Quervain TeFnosynovitis [17, 31]. The measurement of grip and pinch forces and hand performance showed that using both splints reduces these variables. Considering the limitation of thumb movements, this reduction of forces was a logical prediction. However, the production of grip and pinch forces in a palmar splint is more than that of a radial splint. This advantage can be related to the thumb’s closer and more effective interaction with the index finger and other fingers. According to previous studies, it is expected that immobilization inside the splint for a longer period will improve the lesion and ultimately increase the pinch and grip strength in the lesion sufferers [11, 20]. Previous studies have measured upper limb function mainly using the arm, shoulder, and hand disability questionnaires [13, 15, 19, 23, 24, 28, 32].
Since the use of questionnaires for longitudinal studies cannot be used in this study, the Jebsen-Taylor test was used, which includes many daily movements of the upper limbs, and the effect of the limitation of the range of movements and coordination along the movement chain can be measured. The test time did not differ between the two splints. It seems that in this test, the coordinated movements of the upper limb chain are more effective than the grip and pinch strength of the fingers. Therefore, restricting the wrist movements performed in both splints may have slowed down the movements of the manual function test.
The presented results should be interpreted in proportion to the limitations of the present study. It should be noted that the number of study participants is small and most participants had lesions of a chronic type. This study investigated the immediate effect of splints. The splints used in this study were of the thumb forearm spica type, made of hard plastic, and covered to the patients based on the measurements. Due to the limitation of the splints in three sizes, minor movements of the hand inside the splint may have occurred during the measurements.
Conclusion
In the prescription, design, and construction of thumb spica splints for people with de Quervain tenosynovitis, if the thumb is placed in the palmar abduction position, the pain is reduced more effectively. Besides, placing the thumb in the palmar abduction position preserves the strength of grasping objects in the hand and between the fingers to perform manual functions.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences (Code: IR.MUI.REC.1397.379). The informed consent was obtained from each participant before study. The participants were given the permission to cancel their participation at any stage of study. The forms contained the personal information was coded to ensure the confidentiality of information.
Funding
The paper was extracted from the MSc. thesis of the first, Department of Orthotics and Prosthetics, School of Rehabilitation Sciences, Isfahan University of Medical Sciences, Isfahan, Iran (No. 397558).
Authors' contributions
Conceptualization: Ebrahim Sadeghi-Demneh, Hanieh Mohammadzadeh and Abolghasem Zarezadeh; Investigation: Hanieh Mohammadzadeh, Abolghasem Zarezadeh, Mohammad Ali Mardani and Ebrahim Sadeghi-Demneh; Writing-original draft, and writing-review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude from the participants of the research and members of University Research Council.
De Quervain tenosynovitis usually occurs due to inflammation and degenerative changes of the connective tissues in the first extensor compartment of the wrist [1, 2]. In this condition, the tendons of the abductor pollicis longus and extensor pollicis brevis muscles get stuck in the fibrous tunnel due to friction [1]. Although different opinions have been expressed regarding the type of tissue changes that can be the origin of de Quervain syndrome [3], there is a consensus regarding the presence of repetitive movements as the cause of tissue lesions. The onset of tendon involvement in the first extensor compartment of the wrist is accompanied by symptoms such as local pain and tenderness on the radial side of the wrist and the base of the thumb [4]. In people suffering from de Quervain tenosynovitis, holding objects in hand or ulnar deviation of the wrist causes stretching of the involved tissues and intensification of pain [1]. Accordingly, the power to grasp things is reduced, and slowness and inability in manual functions appear [5]. This disorder in manual function can also affect the daily activities of patients with this condition [6, 7].
To treat de Quervain tenosynovitis, non-surgical options are usually preferable [8]. According to scientific and clinical evidence, one of the conservative interventions commonly used for de Quervain tenosynovitis is to control the movements of the lesion site through a thumb splint [9]. Immobilization of the lesion site can be applied alone or with other conservative interventions, such as local injection [10]. For those suffering from de Quervain, a splint called a thumb spica is used, which, while placed on the forearm and wrist areas, surrounds the thumb and its middle joint [11]. The purpose of using the thumb spica splint is to limit the movements in the carpometacarpal and metacarpophalangeal joints of the first finger [12]. Therefore, wearing the thumb spica splint stabilizes the base joints of the thumb and creates a state of rest in the involved tendon [13, 14]. So, using a thumb spica splint is expected to effectively reduce inflammation and accelerate the healing of the lesion site [1, 13].
To treat de Quervain tenosynovitis, the proximal joints of the thumb are immobilized in the abduction position to prevent flexion of the thumb and stretching of the damaged tendons on the carpometacarpal and metacarpophalangeal joints of the first finger [5, 13, 14]. Considering that there are two abduction positions in the thumb (palmar [relatively vertical movement of the thumb away from the surface of the palm] and radial [movement of the thumb parallel to the surface of the palm or the radius bone]), it has not yet been determined which position can be more suitable for thumb spica splint design.
Based on what was discussed, the current study aimed to compare the effect of two types of splints with different positions of abduction (palmar and radial) of the thumb on pain, strength, and hand function in patients with de Quervain tenosynovitis.
Materials and Methods
This research was a quasi-experimental study. The samples were recruited by convenience non-probability sampling. The inclusion criteria included the presence of tenderness in the first extensor compartment of the wrist, the occurrence of pain (higher than score 3 based on the visual analog scale) in the radial part of the wrist, positive Finkelstein test, and extensor pollicis brevis tendon entrapment test [1, 5]. The exclusion criteria included corticosteroid injection in the wrist during the previous 3 months, surgery, fracture, severe osteoporosis, history of splint use, joint arthritis, or peripheral nerve involvement in the upper limb [15]. Also, there was no specific limit for the time of developing the complication, and people with acute and chronic lesions could enter the study. Before recruiting the samples and start the study, an ethical code was obtained, the volunteers were explained the study’s details and their written consent was obtained.
Thirty people with de Quervain tenosynovitis were evaluated in this study. Interventions included with and without splint palmar abduction and with splint radial thumb abduction. Splints kept the wrist at 15 degrees of extension (Figure 1). In the palmar abduction splint, the thumb was placed at 30 degrees of abduction and perpendicular to the palm (Figure 1A). In the radial abduction splint, the thumb was set at 30 degrees of abduction and parallel to the palm (Figure 1B). In splints, the interphalangeal joint of the thumb was outside the splint and moved freely.
The participants’ outcomes of pain intensity, grip strength, lateral pinch, palmar pinch strength, and manual function were measured in this study. The visual analog scale was used to measure pain intensity. People pressed a soft cylinder made of polyethylene foam in their palms. Then it was released, and the amount of pain during squeezing was marked on a 10 cm line. The number 0 means the absence of pain, and 10 means the most intense pain. The grip strength was measured through a hand dynamometer. The person pressed the dynamometer lever (SH5001, SAEHAN Inc., South Korea) with maximum power (Figure 2A) [16]. The pinch force was measured in both lateral and palmar pinches using a pinch gauge (SH5008, SAEHAN Inc., South Korea).
To measure the lateral pinch force, a person uses the pinch gauge as if he was holding a key and puts the maximum force into the movable button of the device with his thumb (Figure 2B). To record the palmar pinch force, the person holds the pinch dynamometer in the position of holding a needle between thumb and index fingers then applies a pinching force by the thumb (Figure 2C) [17]. The Jebsen-Taylor test was used to measure the manual performance of the participants. Jebsen test had seven subcategories (writing, turning over cards, picking up small objects, placing four beads on top of each other, moving light cans, moving heavy cans, and imitating movements while eating) [18]. A timer recorded the test execution time; recording a shorter time meant better manual performance.
The evaluations (except the Jebsen-Taylor evaluation) were repeated three times to reduce the error probability, and the average measurements were calculated and recorded. Statistical analysis was done using SPSS software, version 16. After confirming the normality of the data distribution by the Shapiro-Wilk test, the existence of differences in the study situations was checked by the analysis of variance (ANOVA) with repeated measures. In case of reporting a statistically significant difference between the study conditions, Bonferroni test was used for pairwise comparison of the intervention conditions. A significance level of 0.05 was considered in all tests.
Results
Descriptive statistics are presented in Table 1.
The results of the analysis of the variance test for repeated measures showed statistically significant differences between all study variables (Table 2).
To compare two by two study conditions, Bonferroni test was used in the output of variance analysis (Table 3), which showed that using both types of splints reduced pain.
Using both types of splints has significantly reduced grip, lateral and palmar pinch strength and increased the time to perform the Jebsen-Taylor test. Comparing the two splints showed that the palmar abduction splint is more effective in reducing pain than the radial abduction splint. When using the palmar abduction splint, the grip, palmar pinch, and lateral pinch strength are greater than the radial abduction splint (P<0.001). However, no statistically significant difference was observed in comparing Jebsen test time between the two study splints (P=0.12).
Discussion
The use of plastic splints reduced the pain of de Quervain tenosynovitis. Since the splints limited the range of motion of the hand joints, they also reduced the function of the hand.
The use of thumb spica is one of the most common treatments for de Quervain tenosynovitis [13]. However, previous studies have reported the effectiveness of local injection more than thumb immobilization [19]. Some studies have also used immobilization methods such as bandages [20] and plastering [21]. Due to the definite ineffectiveness of local injection of corticosteroids in some cases, splints can be used as an alternative option or simultaneous with injection [22]. It is necessary to explain that splint treatment is not limited to conservative therapies and can also be used after surgery in patients with de Quervain tenosynovitis [23].
The wide range of applications of thumb splints in the treatment of tenosynovitis highlights the detection of the more effective types of this splint [5]. So far, what has been most important in the design of the thumb splint includes the restriction of wrist movements [24] and excessive movements [25], as well as, to some extent, compliance with the weight [26] and the duration of using the splint [27]. In the current study, in addition to controlling the lateral movements of the wrist, attention was also paid to the position of the thumb inside the splint. Paying attention to the carpometacarpal condition of the thumb in splints was the most important difference between this study and previous studies.
The results of this study showed that the use of splints reduces thumb spica while grasping objects. Reduction of pain following the use of a splint or thumb immobilization was also reported in all previous studies [9, 11, 20, 22, 28, 29]. To make it possible to investigate the immediate effect of the splints in this study, pain intensity was measured while pressing the foam cylinder in the palm to determine the role of the splint in reducing the momentary pressure on the lesion site. During the use of the palmar abduction splint, less pain was reported with the radial abduction splint. However, it cannot be interpreted as a direct result of a palmar abduction splint because the comfort of the position of the thumb inside the splint or the pressure of the edge of the splint on the thumb can also be involved in reporting the intensity of pain. It should also be noted that the report of pain can be influenced by the psychological and personality factors of people as well [30].
Previous studies show that palmar and lateral pinch force measurements are reduced as a reliable and valid variable in de Quervain TeFnosynovitis [17, 31]. The measurement of grip and pinch forces and hand performance showed that using both splints reduces these variables. Considering the limitation of thumb movements, this reduction of forces was a logical prediction. However, the production of grip and pinch forces in a palmar splint is more than that of a radial splint. This advantage can be related to the thumb’s closer and more effective interaction with the index finger and other fingers. According to previous studies, it is expected that immobilization inside the splint for a longer period will improve the lesion and ultimately increase the pinch and grip strength in the lesion sufferers [11, 20]. Previous studies have measured upper limb function mainly using the arm, shoulder, and hand disability questionnaires [13, 15, 19, 23, 24, 28, 32].
Since the use of questionnaires for longitudinal studies cannot be used in this study, the Jebsen-Taylor test was used, which includes many daily movements of the upper limbs, and the effect of the limitation of the range of movements and coordination along the movement chain can be measured. The test time did not differ between the two splints. It seems that in this test, the coordinated movements of the upper limb chain are more effective than the grip and pinch strength of the fingers. Therefore, restricting the wrist movements performed in both splints may have slowed down the movements of the manual function test.
The presented results should be interpreted in proportion to the limitations of the present study. It should be noted that the number of study participants is small and most participants had lesions of a chronic type. This study investigated the immediate effect of splints. The splints used in this study were of the thumb forearm spica type, made of hard plastic, and covered to the patients based on the measurements. Due to the limitation of the splints in three sizes, minor movements of the hand inside the splint may have occurred during the measurements.
Conclusion
In the prescription, design, and construction of thumb spica splints for people with de Quervain tenosynovitis, if the thumb is placed in the palmar abduction position, the pain is reduced more effectively. Besides, placing the thumb in the palmar abduction position preserves the strength of grasping objects in the hand and between the fingers to perform manual functions.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences (Code: IR.MUI.REC.1397.379). The informed consent was obtained from each participant before study. The participants were given the permission to cancel their participation at any stage of study. The forms contained the personal information was coded to ensure the confidentiality of information.
Funding
The paper was extracted from the MSc. thesis of the first, Department of Orthotics and Prosthetics, School of Rehabilitation Sciences, Isfahan University of Medical Sciences, Isfahan, Iran (No. 397558).
Authors' contributions
Conceptualization: Ebrahim Sadeghi-Demneh, Hanieh Mohammadzadeh and Abolghasem Zarezadeh; Investigation: Hanieh Mohammadzadeh, Abolghasem Zarezadeh, Mohammad Ali Mardani and Ebrahim Sadeghi-Demneh; Writing-original draft, and writing-review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude from the participants of the research and members of University Research Council.
References
- Ilyas AM, Ast M, Schaffer AA, Thoder J. De quervain tenosynovitis of the wrist. The Journal of the American Academy of Orthopaedic Surgeons. 2007; 15(12):757-64. [DOI:10.5435/00124635-200712000-00009] [PMID]
- VuilleVuillemin V, Guerini H, Bard H, Morvan G. Stenosing tenosynovitis. Journal of Ultrasound. 2012; 15(1):20-8. [DOI:10.1016/j.jus.2012.02.002] [PMID] [PMCID]
- Adams JE, Habbu R. Tendinopathies of the hand and wrist. Journal of the American Academy of Orthopaedic Surgeons. 2015; 23(12):741-50. [DOI:10.5435/JAAOS-D-14-00216] [PMID]
- Keir PJ, Farias Zuniga A, Mulla DM, Somasundram KG. Relationships and mechanisms between occupational risk factors and distal upper extremity disorders. Human factors. 2021; 63(1):5-31. [DOI:10.1177/0018720819860683] [PMID]
- Scott A, Backman LJ, Speed C. Tendinopathy: Update on pathophysiology. The Journal of Orthopaedic and Sports Physical Therapy. 2015; 45(11):833-41. [DOI:10.2519/jospt.2015.5884] [PMID]
- Satteson E, Tannan SC. De quervain tenosynovitis. Treasure Island (FL): StatPearls Publishing; 2021. [PMID]
- Afshar A, Tabrizi A. Pregnancy-related hand and wrist problems. The Archives of Bone and Joint Surgery. 2021; 9(3):345-49. [DOI:10.22038/abjs.2020.50995.2531] [PMID]
- Wolf JM, Sturdivant RX, Owens BD. Incidence of de quervain's tenosynovitis in a young, active population. The Journal of Hand Surgery. 2009; 34(1):112-5. [DOI:10.1016/j.jhsa.2008.08.020] [PMID]
- Huisstede BM, Coert JH, Fridén J, Hoogvliet P; European HANDGUIDE Group. Consensus on a multidisciplinary treatment guideline for de quervain disease: results from the European HANDGUIDE study. Physical Therapy. 2014; 94(8):1095-110. [DOI:10.2522/ptj.20130069] [PMID]
- Novikov AV, Shchedrina MA, Petrov SV. De Quervain’s disease (etiology, pathogenesis, diagnosis and treatment). Part I. N.N. Priorov Journal of Traumatology and Orthopedics. 2019; 26(3):54-62. [DOI:10.17116/vto201903154]
- Kang HJ, Koh IH, Jang JW, Choi YR. Endoscopic versus open release in patients with de quervain's tenosynovitis: A randomised trial. The Bone & Joint Journal. 2013; 95-B(7):947-51. [DOI:10.1302/0301-620X.95B7.31486] [PMID]
- Larsen CG, Fitzgerald MJ, Nellans KW, Lane LB. Management of de quervain tenosynovitis: A critical analysis review. JBJS Reviews. 2021; 9(9):e21. [DOI:10.2106/JBJS.RVW.21.00069] [PMID]
- Goel R, Abzug JM. De Quervain's tenosynovitis: A review of the rehabilitative options. Hand. 2015; 10(1):1-5. [DOI:10.1007/s11552-014-9649-3] [PMID] [PMCID]
- Coldham F. The use of splinting in the non-surgical treatment of de quervain’s disease: A review of the literature. The British Journal of Hand Therapy. 2006; 11(2):48-55. [DOI:10.1177/175899830601100203]
- Nemati Z, Javanshir MA, Saeedi H, Farmani F, Aghajani Fesharaki S. The effect of new dynamic splint in pinch strength in de quervain syndrome: A comparative study. Disability and rehabilitation. Assistive Technology. 2017; 12(5):457-61. [DOI:10.3109/17483107.2016.1139635] [PMID]
- Hengwei F, Zifang H, Qifei W, Weiqing T, Nali D, Ping Y, et al. Prevalence of idiopathic scoliosis in chinese schoolchildren: A large, population-based study. Spine. 2016; 41(3):259-64. [DOI:10.1097/BRS.0000000000001197] [PMID]
- Huisstede BM, Gladdines S, Randsdorp MS, Koes BW. Effectiveness of conservative, surgical, and postsurgical interventions for trigger finger, dupuytren disease, and de quervain disease: A systematic review. Archives of Physical Medicine and Rehabilitation. 2018; 99(8):1635-49. [DOI:10.1016/j.apmr.2017.07.014]
- Ishii S, Sairyo K. Analysing orthotic designs for de Quervain’s disease based on in vivo gliding distance of extensor pollicis brevis tendon. International Journal of Therapy and Rehabilitation. 2018; 25(2):51-7. [DOI:10.12968/ijtr.2018.25.2.51]
- Huang TH, Feng CK, Gung YW, Tsai MW, Chen CS, Liu CL. Optimization design of thumbspica splint using finite element method. Medical & Biological Engineering & Computing. 2006; 44(12):1105-11. [DOI:10.1007/s11517-006-0131-4] [PMID]
- Chu CH, Wang IJ, Sun JR, Liu CH. Customized designs of short thumb orthoses using 3D hand parametric models. Assistive Technology. 2022; 34(1):104-11. [DOI:10.1080/10400435.2019.1709917] [PMID]
- Chow KKC. Splint for de quervain disease: A new design. Hong Kong Journal of Occupational Therapy. 2009; 19(1):31-32. [DOI:10.1016/S1569186109700427]
- Mardani-Kivi M, Karimi Mobarakeh M, Bahrami F, Hashemi-Motlagh K, Saheb-Ekhtiari K, Akhoondzadeh N. Corticosteroid injection with or without thumb spica cast for de quervain tenosynovitis. The Journal of Hand Surgery. 2014; 39(1):37-41. [DOI:10.1016/j.jhsa.2013.10.013] [PMID]
- Richie CA 3rd, Briner WW Jr. Corticosteroid injection for treatment of de quervain's tenosynovitis: A pooled quantitative literature evaluation. The Journal of the American Board of Family Practice 2003; 16(2):102-6. [DOI:10.3122/jabfm.16.2.102] [PMID]
- Ippolito JA, Hauser S, Patel J, Vosbikian M, Ahmed I. Nonsurgical treatment of de quervain tenosynovitis: A prospective randomized trial. Hand. 2020; 15(2):215-19. [DOI:10.1177/1558944718791187] [PMID] [PMCID]
- Lang KR, Gibson BS, Oppenhuizen KM. Conservative treatment of de quervain’s tenosynovitis in occupational therapy: A retrospective outcome study. Allendale: Grand Valley State University; 2014. [Link]
- Menendez ME, Thornton E, Kent S, Kalajian T, Ring D. A prospective randomized clinical trial of prescription of full-time versus as-desired splint wear for de quervain tendinopathy. International Orthopaedics. 2015; 39(8):1563-9. [DOI:10.1007/s00264-015-2779-6] [PMID]
- Başar B, Aybar A, Basar G, Başar H. The effectiveness of corticosteroid injection and splint in diabetic de quervain’s tenosynovitis patients: A single-blind, randomized clinical consort study. Medicine. 2021; 100(35):e27067. [DOI:10.1097/MD.0000000000027067] [PMID] [PMCID]
- Haghighat S, Vahdatpour B, Ataei E. The Effect of extracorporeal shockwave therapy on de Quervain tenosynovitis; a clinical trial. Shiraz E-Medical Journal. 2021; 22(8):e106559. [DOI:10.5812/semj.106559]
- Awan WA, Babur MN, Masood T. Effectiveness of therapeutic ultrasound with or without thumb spica splint in the management of De Quervain's disease. Journal of Back and Musculoskeletal Rehabilitation. 2017; 30(4):691-7. [DOI:10.3233/BMR-160591] [PMID]
- Abi-Rafeh J, Kazan R, Safran T, Thibaudeau S. Conservative management of de quervain stenosing tenosynovitis: Review and presentation of treatment algorithm. Plastic and Reconstructive Surgery. 2020; 146(1):105-26. [DOI:10.1097/PRS.0000000000006901] [PMID]
- Barati H, Zarezadeh A, MacDermid JC, Sadeghi-Demneh E. The immediate sensorimotor effects of elbow orthoses in patients with lateral elbow tendinopathy: A prospective crossover study. Journal of Shoulder and Elbow Surgery. 2019; 28(1):e10-17. [DOI:10.1016/j.jse.2018.08.042] [PMID]
- Fournier K, Bourbonnais D, Bravo G, Arsenault J, Harris P, Gravel D. Reliability and validity of pinch and thumb strength measurements in de Quervain's disease. Journal of Hand Therapy. 2006; 19(1):2-10, quiz 11. [DOI:10.1197/j.jht.2005.10.002] [PMID]
- DeMatteo C, Law M, Russell D, Pollock N, Rosenbaum P, Walter S. The reliability and validity of the quality of upper extremity skills test. Physical & Occupational Therapy in Pediatrics. 1993; 13(2):1-18. [DOI:10.1080/J006v13n02_01]
- Ashraf MO, Devadoss VG. Systematic review and meta-analysis on steroid injection therapy for de Quervain's tenosynovitis in adults. European Journal of Orthopaedic Surgery & Traumatology. 2014; 24(2):149-57. [DOI:10.1007/s00590-012-1164-z] [PMID]
- Jongprasitkul H., Suputtitada A., Kitisomprayoonkul W., Pintawiruj K.. Elastic bandage vs. neoprene thumb stabilizer splint in acute De Quervain’s tenosynovitis. Asian Biomedicine. 2017; 5(2): 263-7. [DOI:10.5372/1905-7415.0502.035]
- Mehdinasab SA, Alemohammad SA. Methylprednisolone acetate injection plus casting versus casting alone for the treatment of de Quervain's tenosynovitis. Archives of Iranian Medicine. 2010; 13(4):270-4. [PMID] [Link].
- Allbrook V. 'The side of my wrist hurts': De Quervain's tenosynovitis. Australian Journal of General Practice. 2019; 48(11):753-6. [DOI:10.31128/AJGP-07-19-5018] [PMID]
- Dominick KL, Jordan JM, Renner JB, Kraus VB. Relationship of radiographic and clinical variables to pinch and grip strength among individuals with osteoarthritis. Arthritis and Rheumatism. 2005; 52(5):1424-30. [DOI:10.1002/art.21035] [PMID]
- Lane LB, Boretz RS, Stuchin SA. Treatment of de Quervain's disease:role of conservative management. Journal of Hand Surgery (Edinburgh, Scotland). 2001; 26(3):258-60. [DOI:10.1054/jhsb.2001.0568] [PMID]
- Vranceanu A-M, Jupiter JB, Mudgal CS, Ring D. Predictors of pain intensity and disability after minor hand surgery. The Journal of Hand Surgery. 2010; 35(6):956-60. [DOI:10.1016/j.jhsa.2010.02.001] [PMID]
- Forget N, Piotte F, Arsenault J, Harris P, Bourbonnais D. Bilateral thumb's active range of motion and strength in de Quervain's disease: comparison with a normal sample. Journal of Hand Therapy. 2008; 21(3):276-84. [DOI:10.1197/j.jht.2008.03.004] [PMID]
Type of Study: Applicable |
Subject:
Orthotics & Prosthetics
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
