

Volume 24, Issue 3 (Autumn 2023)
jrehab 2023, 24(3): 308-327 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Vahidi H, AkbarFahimi N, Rahmani A, Rassafiani M. The Effects of Islamic Culture on the Occupational Performance of Clients Receiving Occupational Therapy in Islamic Countries: A Review Study With Content Analysis Approach. jrehab 2023; 24 (3) :308-327
URL: http://rehabilitationj.uswr.ac.ir/article-1-3232-en.html
URL: http://rehabilitationj.uswr.ac.ir/article-1-3232-en.html



1- Department of Occupational Therapy , School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran., The University of Social Welfare and Rehabilitation sciences
2- Department of Occupational Therapy , School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,fahimi1970@yahoo.com
3- Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran., Nursing Faculty, Tabriz University of Medical Sciences
4- School of Allied Health, Exercise and Sports Sciences, Charles Sturt University, Albury, Australia., School of Allied Health, Exercise and Sports Sciences, Charles Sturt University, Albury, Australia
2- Department of Occupational Therapy , School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
3- Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran., Nursing Faculty, Tabriz University of Medical Sciences
4- School of Allied Health, Exercise and Sports Sciences, Charles Sturt University, Albury, Australia., School of Allied Health, Exercise and Sports Sciences, Charles Sturt University, Albury, Australia
Full-Text [PDF 3469 kb]
(1494 Downloads)
| Abstract (HTML) (7121 Views)
Full-Text: (2458 Views)
Introduction
Occupational therapy aims to develop treatment approaches and outcomes consistent with the lifestyle and values of clients. So, the culture of the client and the therapist, as well as their interactions, play crucial roles in the adjustment of the client’s lifestyle and value system [1].
Islamic culture holds prevailing in the Islamic Middle East countries. However, these countries exhibit many differences in historical evolution, social composition, and economic structures [4]. The cultural system of Muslims in the Middle East has a rich order intertwined with a set of Islamic and local customs [5]. According to Lee Bowen, the daily life of people in this cultural context is a blend of modernity and tradition, where classical and local religious traditions converge to address various problems, such as finding a job, raising children, eliminating strife in a community, fighting inflation, and solving economic problems. In this everyday arena, people grapple with cultural conflicts between tradition and modernity or religiosity and secularism, created by rapid changes in the Middle East [5].
Although occupational therapy professional frameworks have been developed and accepted in Western countries, few studies have explored its appropriateness and application for different cultural groups [7]. These frameworks for occupational therapy have evolved in the context of Western values that focus on individualism, autonomy, competence, and mastery [8, 9].
Awaad (2003) cautioned against imposing Western concepts of occupational therapy practices on cultures with profoundly distinct beliefs, values, and attitudes, highlighting the potential danger and risks of being inappropriate or irrelevant to the situations in those different cultures. This issue may even lead to conceptual and philosophical conflicts. The crux of the matter lies in the emphasis of Western care models on bolstering individual independence, contrary to Eastern and Islamic paradigmatic beliefs that focus on fatalism and family responsibilities [2].
Since the cultural context significantly influences occupational choices and behaviors rooted in societal beliefs, values, and expectations, occupational therapists should consider their clients’ culture during their assessment and intervention planning [10]. Although research studies have delved into the impact of culture on occupational performance within specific cultural contexts, and there are some references to these cases in various sources of occupational therapy [10, 13], limited attention has been directed toward the relationship between Islamic culture and occupational performance. Of course, studies have been conducted in Islamic countries [14-16], and among Muslim immigrants living in non-Islamic countries [17], they have yet to culminate in a comprehensive guide for occupational therapists. This review aims to provide insight for researchers and occupational therapists regarding the effects of Islamic culture on occupational therapy. Therefore, this study sheds light on the impact of Islamic culture on the occupational performance of occupational therapy clients in Islamic countries.
Materials and Methods
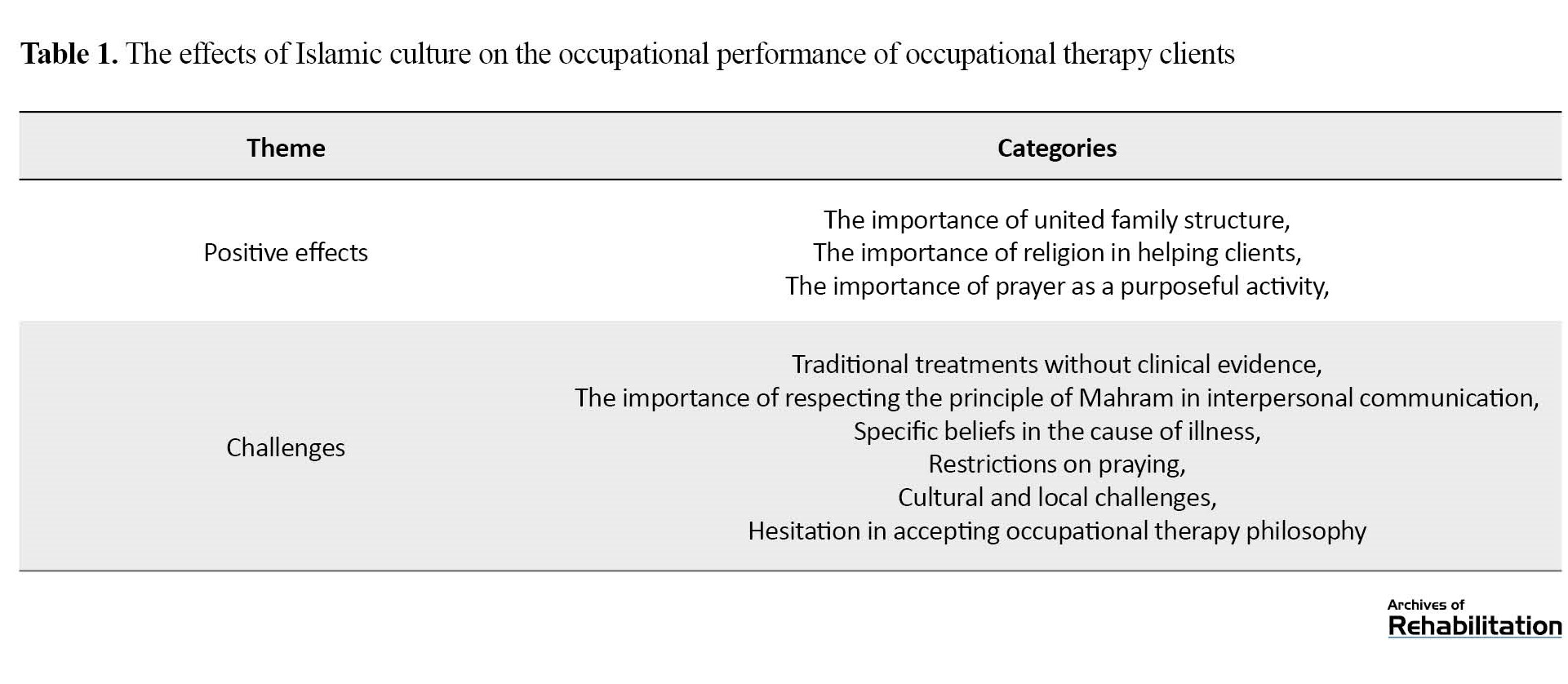
This study investigates the articles related to the effects of Islamic culture on the occupational performance of clients receiving occupational therapy using the explicit content analysis method. Kassarjian (1977) highlighted that content analysis should follow a clear and purposeful process structure [20]. Accordingly, our study adopts the 4-step process model derived from Meiring’s model (2008): Collecting articles, descriptive analysis, choosing classes and categories, and evaluating materials and research methods [21]. In line with this approach, the related articles were collected. Then, they were reviewed and descriptively analyzed by the researchers. A total of 39 primary codes were extracted from them. Next, these concepts and codes were classified based on their similarities and differences, and primary classes were formed. Later, these initial classes were grouped, and the final classes were created. Table 1 provides an overview of all analytical categories and their definitions.
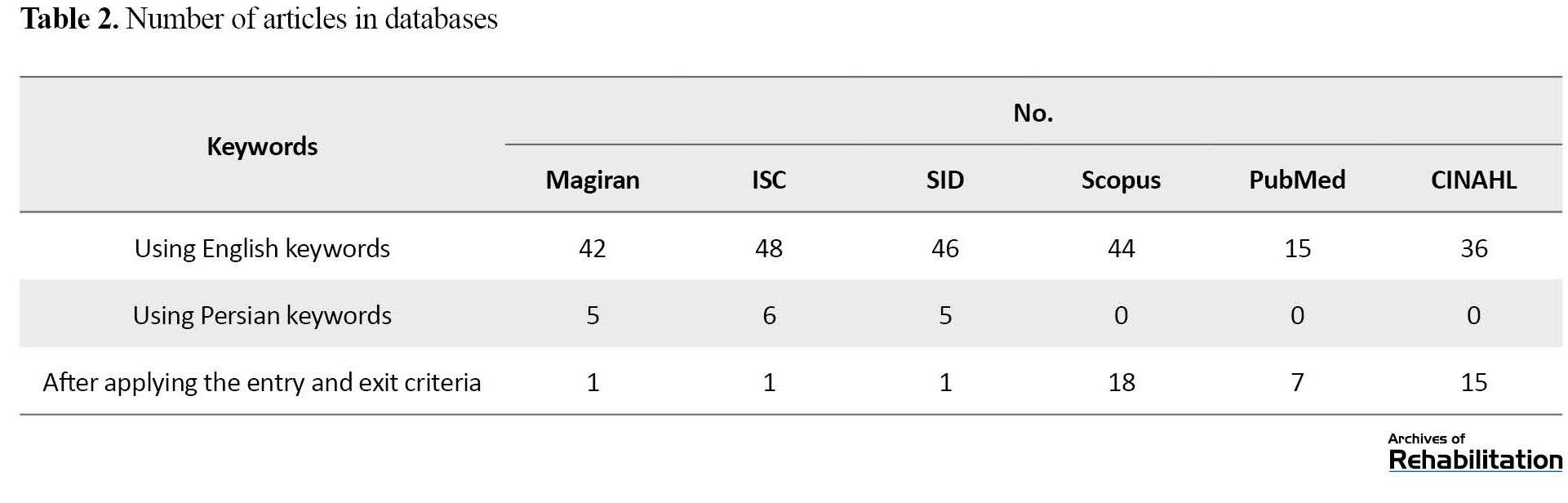
Literature review was conducted in CINAHL, Scopus, PubMed, SID, ISC, Magiran, and Google Scholar (Table 2).
The inclusion criteria are outlined in Table 3.
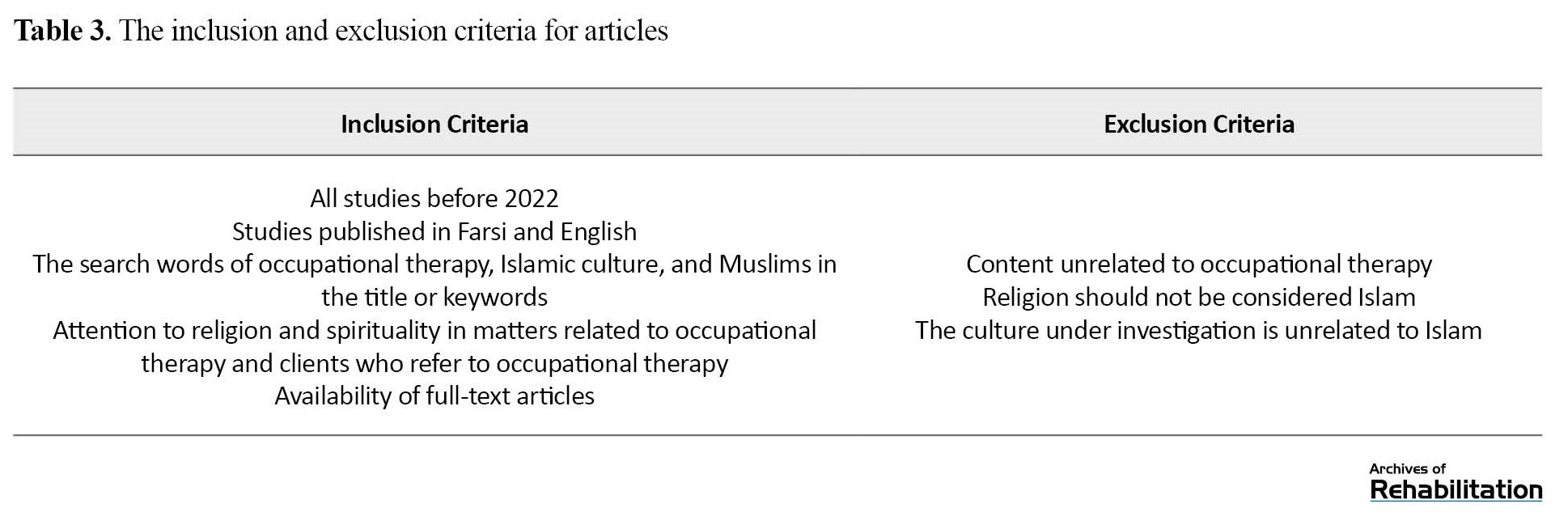
The limited number of studies in the field of Islamic culture and occupational therapy was the reason for choosing articles from all periods. The keywords used for the literature search were occupational therapy, Islamic culture, and Muslims, with their equivalents in Persian. At first, 46 articles were extracted; many were about spirituality and culture. After reviewing all of them, according to the purpose of the research, only articles related to occupational therapy in the Islamic cultural context were selected, resulting in 20 articles.
Evaluation of research materials and methods
To enhance the credibility and quality assessment, the critical appraisal skills program (CASP) tool was employed [35], consisting of 10 questions to evaluate the quality of studies. The results of this study have been presented and discussed to obtain some practical guidelines for nursing researchers of Tabriz University of Medical Sciences and Occupational Therapy Department of Tabriz University of Medical Sciences and University of Rehabilitation Sciences and Social Health. A classification scheme with predefined categories and clear definitions, coupled with coding reliability, increased the internal validity of the findings. Decontextualization and theory-based abstraction from the content analysis results provide a certain degree of generalization of the findings, consequently bolstering external validity [36]. In addition, this study has incorporated strategies for building trust in qualitative research. The authors read the articles independently and, time after time, discussed them while analyzing categories and units of meaning until they reached a consensus.
Results
Analyzing the available articles has finally created two general themes: Positive effects and challenges. These themes encapsulate the impact of Islamic culture on the occupational performance of clients receiving occupational therapy (Table 1).
Positive effects
Positive effects refer to all the opportunities and positive factors that Islamic culture in Muslim countries can influence the performance of occupational therapy. Occupational therapists can harness these opportunities during the visit of these clients and integrate them into the evaluation and treatment of their clients so that they can provide services that are completely in line with the client’s culture, beliefs, and customs. This topic itself is divided into four categories, all of which are discussed below.
The importance of united family structure
In Eastern countries, especially in the Middle East, the family system is completely collectivist, creating a strong unity and connection between family members. Each person in this family is assigned a special and strong role. For example, despite a patriarchal system in this culture, women also assume leadership at the head of family management affairs, actively participate in all family decisions and maintain family cohesion. Family and caregivers help in all matters of clients and play the role of facilitators. They participate in all treatment stages, both for adults and children.
The importance of religion in helping clients
According to the guidelines in the Holy Quran and the words of Prophet Muhammad, Islam offers many recommendations for the prevention and treatment of diseases. It also holds positive attributes to help care for patients. For example, Islamic teachings emphasize the integration of body and mind, the stress-reducing effect of faith and belief in the afterlife, believing in Islamic commands to protect the physical well-being, Islam’s humane approach in reducing stigma, trusting God in the results of affairs, and the role of Islam in reducing social harms such as suicide and drug and alcohol use.
The importance of prayer as a purposeful activity
Prayer represents a daily religious and spiritual activity Muslims do as a mandatory activity. Most studies reviewed realized the potential of prayer as a targeted activity to improve gross motor skills and cognitive abilities. From a psychological standpoint, prayer can serve as a source of support for most disorders, including stroke.
Challenges
Challenges comprise a series of obstacles and limitations that hinder the performance of occupational therapy and can reduce the quality of services. These challenges include the following categories, which will be discussed in detail about each of them.
Traditional treatments without clinical evidence
In Islamic countries, it is common to see some treatments often without clinical evidence. They are often rooted in superstitions and lack official or unofficial proven sources. These treatments do not exist in religious reference books.
The importance of respecting the principle of Mahram in interpersonal communication
In Muslim societies, interpersonal communication is well-defined, and everyone must obey them. In Islam, doctors, therapists, and nurses are considered Mahram for patients. It means they have permission to touch the patient’s body for therapeutic purposes. This problem can be considered a challenge, particularly when teaching self-care activities such as dressing, going to the toilet, or bathing. Considering the cohesive structure of families, the therapist may involve the patient’s caregivers in training.
Specific beliefs in the cause of illness
Superstitions in the origin of diseases in Islamic countries pose one of the biggest challenges for the treatment staff. It not only interferes with occupational therapy but also causes harm to the clients. In current medical science, the cause of most diseases is generally attributed to genetics, microbes, chemical agents, etc. each with scientifically proven reasons. However, clients talk about beliefs that are mostly superstitious about the cause of the disease.
Restrictions on praying
To engage in prayer, clients should wash some parts of their body, such as their face, hands, and feet, followed by saying the prayer, which includes large standing and sitting movements. This purposeful activity may be disturbed due to physical disorders. For example, a person with a brain vascular injury in the acute phase can hardly, if impossible, do the prayer.
Cultural and local challenges
Occupational therapy researchers have noted the absence of local assessment tools based on native culture. These tools include the evaluation of all daily life activities of the clients in the fields of occupational therapy, spirituality, and religion. The next challenge pertains to the clients’ clothes, often based on Islamic culture. Full hijab is observed for both women and men. In this context, one of the challenges is the large number of clothes so that they can observe hijab in the family and the society.
Hesitation in accepting occupational therapy philosophy
One of the important philosophies of occupational therapy revolves around using occupation and activity to treat the patient’s disability. Most of these activities include self-care, work, and leisure. According to several reviewed studies, occupational therapists’ challenges in Islamic countries are the desire for treatments that have faster results, including aggressive approaches, drug therapy, or sports-based interventions, which are less common in occupational therapists.
Discussion
The findings of this study illuminate the relationship between cultural context and the occupational performance of clients undergoing occupational therapy. It is evident that people’s occupational performance unfolds within a special environment and context, shaped and colored by various factors in any given society.
The positive effects of Islamic culture represent crucial factors that improve clients’ performance. Occupational therapists can leverage these factors to increase the independence of their clients and support them. In Islamic countries, family members and their unison often support the disabled person and form a backbone for improving the skills of people with disabilities through family assistance. Disruption of this support network can seriously damage the rehabilitation program. From a religious perspective, all the orders of Islam protect the family. Our study findings were consistent with the study of Anoushka (2019). In his research, Islam was found to be an important aspect of the participants’ lives. Many people conduct their daily activities and plan their families based on deep faith in God and his ability to protect them. The Islamic beliefs of the research participants regarded God as the ultimate decision-maker. They believed God had determined birth, death, marriage, and even employment [38].
Islam helps clients in different ways. For example, Islamic commands protect the body, prevent diseases, and help reduce stress and anxiety. Saged et al. (2022) stated that the Islamic religion-based interventions would significantly lower levels of depression and anxiety among participants. Also, a significant improvement in the patient’s general health was observed after the intervention. The participants were satisfied and believed everything that happened to them was predestined [39].
One of the important categories regarding positive opportunities to improve movement and other daily life skills is to observe prayers, which are highly valued in Islamic countries. Occupational therapists can use this opportunity to implement targeted skills and activities. The effects of prayer can be examined in various fields, for example, motor skills, brain activity, and other documented health benefits in multiple articles [40, 41, 42].
Cultural challenges pose obstacles to providing occupational therapy services, which must be dealt with delicately and require appropriate solutions. One of the cultural challenges is the respect for the principle of Mahram in interpersonal communication. Our findings were consistent with Caroline Murray’s study. From her point of view, the structure of social and cultural challenges, such as the social behaviors of occupational therapists and their norms, values, and beliefs, are vital [43].
Another important challenge in the treatment and rehabilitation of occupational therapy of clients revolves around certain beliefs about the cause of illness, which can create a serious challenge in providing services. Superstitious beliefs are rooted in factors such as a lack of awareness of natural events, environmental control, or fatalistic thinking [45].
The next challenge is the problems and limitations associated with prayers. This challenge, in some ways, may require a lot of effort and struggle on the part of clients or caregivers. It is stated in the Islamic rulings that prayer remains valid under any circumstances [46]. Ravari et al. highlighted that the failure of patients to pray may be due to the conditions of the hospital and related obstacles. These obstacles include the preparations for prayer, the patient’s movement status, and disease-related factors. Based on his study, patients who were aware of prayer rules during illness were more successful in performing the prayer [48].
The next challenge is doubt in accepting occupational therapy philosophy. As mentioned, a very important factor that determines people’s occupational performance is the environmental context that governs that society. In occupational therapy, this context is also an inevitable and effective factor in service delivery [49]. Considering that Iran has a special environmental context and due to this problem and some implementation problems, the use of occupation-based methods faces problems. Thus, clients and therapists prefer body function and structure-based methods due to the objectiveness of goals [50, 51]. A study conducted by Raji et al (2019) in Iran concluded that Iranian occupational therapists prioritized body function in children with cerebral palsy, with the activities of daily living and participation in society as their next priorities [52].
Many cultural challenges are due to the lack of a suitable cultural model based on the Islamic culture of Muslim countries. Actually, one of the appropriate solutions to these challenges can be study and research in this field. Additionally, strengthening the clinical reasoning of occupational therapists can be another useful step in this matter [43].
Conclusion
According to the analysis of the data obtained from the review of the articles, it is evident that Islam, a unique culture in Islamic countries, exerts profound effects on the daily life of occupational therapy clients. These effects can contribute positively and unite families during crises and illness. They also encompass the power of positive thoughts and recommendations to protect and support the disabled person. However, a series of challenges may cause obstacles in people’s daily lives and can even disrupt the treatment and rehabilitation of clients. Occupational therapists can employ these cultural opportunities to improve clients’ performance. Altogether, much research should be conducted to find a suitable model that occupational therapists employ for clinical reasoning to solve these challenges.
Ethical Considerations
Compliance with ethical guidelines
This article is a Meta synthesis with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, data analysis, writing, editing & review: All authors; Data collection: Hassan Vahidi and Nazila Akbar Fahimi; Supervision: Nazila Akbar Fahimi.
Conflict of interest
The authors declared no conflict of interest.
References
Occupational therapy aims to develop treatment approaches and outcomes consistent with the lifestyle and values of clients. So, the culture of the client and the therapist, as well as their interactions, play crucial roles in the adjustment of the client’s lifestyle and value system [1].
Islamic culture holds prevailing in the Islamic Middle East countries. However, these countries exhibit many differences in historical evolution, social composition, and economic structures [4]. The cultural system of Muslims in the Middle East has a rich order intertwined with a set of Islamic and local customs [5]. According to Lee Bowen, the daily life of people in this cultural context is a blend of modernity and tradition, where classical and local religious traditions converge to address various problems, such as finding a job, raising children, eliminating strife in a community, fighting inflation, and solving economic problems. In this everyday arena, people grapple with cultural conflicts between tradition and modernity or religiosity and secularism, created by rapid changes in the Middle East [5].
Although occupational therapy professional frameworks have been developed and accepted in Western countries, few studies have explored its appropriateness and application for different cultural groups [7]. These frameworks for occupational therapy have evolved in the context of Western values that focus on individualism, autonomy, competence, and mastery [8, 9].
Awaad (2003) cautioned against imposing Western concepts of occupational therapy practices on cultures with profoundly distinct beliefs, values, and attitudes, highlighting the potential danger and risks of being inappropriate or irrelevant to the situations in those different cultures. This issue may even lead to conceptual and philosophical conflicts. The crux of the matter lies in the emphasis of Western care models on bolstering individual independence, contrary to Eastern and Islamic paradigmatic beliefs that focus on fatalism and family responsibilities [2].
Since the cultural context significantly influences occupational choices and behaviors rooted in societal beliefs, values, and expectations, occupational therapists should consider their clients’ culture during their assessment and intervention planning [10]. Although research studies have delved into the impact of culture on occupational performance within specific cultural contexts, and there are some references to these cases in various sources of occupational therapy [10, 13], limited attention has been directed toward the relationship between Islamic culture and occupational performance. Of course, studies have been conducted in Islamic countries [14-16], and among Muslim immigrants living in non-Islamic countries [17], they have yet to culminate in a comprehensive guide for occupational therapists. This review aims to provide insight for researchers and occupational therapists regarding the effects of Islamic culture on occupational therapy. Therefore, this study sheds light on the impact of Islamic culture on the occupational performance of occupational therapy clients in Islamic countries.
Materials and Methods
This study investigates the articles related to the effects of Islamic culture on the occupational performance of clients receiving occupational therapy using the explicit content analysis method. Kassarjian (1977) highlighted that content analysis should follow a clear and purposeful process structure [20]. Accordingly, our study adopts the 4-step process model derived from Meiring’s model (2008): Collecting articles, descriptive analysis, choosing classes and categories, and evaluating materials and research methods [21]. In line with this approach, the related articles were collected. Then, they were reviewed and descriptively analyzed by the researchers. A total of 39 primary codes were extracted from them. Next, these concepts and codes were classified based on their similarities and differences, and primary classes were formed. Later, these initial classes were grouped, and the final classes were created. Table 1 provides an overview of all analytical categories and their definitions.
Literature review was conducted in CINAHL, Scopus, PubMed, SID, ISC, Magiran, and Google Scholar (Table 2).
The inclusion criteria are outlined in Table 3.
The limited number of studies in the field of Islamic culture and occupational therapy was the reason for choosing articles from all periods. The keywords used for the literature search were occupational therapy, Islamic culture, and Muslims, with their equivalents in Persian. At first, 46 articles were extracted; many were about spirituality and culture. After reviewing all of them, according to the purpose of the research, only articles related to occupational therapy in the Islamic cultural context were selected, resulting in 20 articles.
Evaluation of research materials and methods
To enhance the credibility and quality assessment, the critical appraisal skills program (CASP) tool was employed [35], consisting of 10 questions to evaluate the quality of studies. The results of this study have been presented and discussed to obtain some practical guidelines for nursing researchers of Tabriz University of Medical Sciences and Occupational Therapy Department of Tabriz University of Medical Sciences and University of Rehabilitation Sciences and Social Health. A classification scheme with predefined categories and clear definitions, coupled with coding reliability, increased the internal validity of the findings. Decontextualization and theory-based abstraction from the content analysis results provide a certain degree of generalization of the findings, consequently bolstering external validity [36]. In addition, this study has incorporated strategies for building trust in qualitative research. The authors read the articles independently and, time after time, discussed them while analyzing categories and units of meaning until they reached a consensus.
Results
Analyzing the available articles has finally created two general themes: Positive effects and challenges. These themes encapsulate the impact of Islamic culture on the occupational performance of clients receiving occupational therapy (Table 1).
Positive effects
Positive effects refer to all the opportunities and positive factors that Islamic culture in Muslim countries can influence the performance of occupational therapy. Occupational therapists can harness these opportunities during the visit of these clients and integrate them into the evaluation and treatment of their clients so that they can provide services that are completely in line with the client’s culture, beliefs, and customs. This topic itself is divided into four categories, all of which are discussed below.
The importance of united family structure
In Eastern countries, especially in the Middle East, the family system is completely collectivist, creating a strong unity and connection between family members. Each person in this family is assigned a special and strong role. For example, despite a patriarchal system in this culture, women also assume leadership at the head of family management affairs, actively participate in all family decisions and maintain family cohesion. Family and caregivers help in all matters of clients and play the role of facilitators. They participate in all treatment stages, both for adults and children.
The importance of religion in helping clients
According to the guidelines in the Holy Quran and the words of Prophet Muhammad, Islam offers many recommendations for the prevention and treatment of diseases. It also holds positive attributes to help care for patients. For example, Islamic teachings emphasize the integration of body and mind, the stress-reducing effect of faith and belief in the afterlife, believing in Islamic commands to protect the physical well-being, Islam’s humane approach in reducing stigma, trusting God in the results of affairs, and the role of Islam in reducing social harms such as suicide and drug and alcohol use.
The importance of prayer as a purposeful activity
Prayer represents a daily religious and spiritual activity Muslims do as a mandatory activity. Most studies reviewed realized the potential of prayer as a targeted activity to improve gross motor skills and cognitive abilities. From a psychological standpoint, prayer can serve as a source of support for most disorders, including stroke.
Challenges
Challenges comprise a series of obstacles and limitations that hinder the performance of occupational therapy and can reduce the quality of services. These challenges include the following categories, which will be discussed in detail about each of them.
Traditional treatments without clinical evidence
In Islamic countries, it is common to see some treatments often without clinical evidence. They are often rooted in superstitions and lack official or unofficial proven sources. These treatments do not exist in religious reference books.
The importance of respecting the principle of Mahram in interpersonal communication
In Muslim societies, interpersonal communication is well-defined, and everyone must obey them. In Islam, doctors, therapists, and nurses are considered Mahram for patients. It means they have permission to touch the patient’s body for therapeutic purposes. This problem can be considered a challenge, particularly when teaching self-care activities such as dressing, going to the toilet, or bathing. Considering the cohesive structure of families, the therapist may involve the patient’s caregivers in training.
Specific beliefs in the cause of illness
Superstitions in the origin of diseases in Islamic countries pose one of the biggest challenges for the treatment staff. It not only interferes with occupational therapy but also causes harm to the clients. In current medical science, the cause of most diseases is generally attributed to genetics, microbes, chemical agents, etc. each with scientifically proven reasons. However, clients talk about beliefs that are mostly superstitious about the cause of the disease.
Restrictions on praying
To engage in prayer, clients should wash some parts of their body, such as their face, hands, and feet, followed by saying the prayer, which includes large standing and sitting movements. This purposeful activity may be disturbed due to physical disorders. For example, a person with a brain vascular injury in the acute phase can hardly, if impossible, do the prayer.
Cultural and local challenges
Occupational therapy researchers have noted the absence of local assessment tools based on native culture. These tools include the evaluation of all daily life activities of the clients in the fields of occupational therapy, spirituality, and religion. The next challenge pertains to the clients’ clothes, often based on Islamic culture. Full hijab is observed for both women and men. In this context, one of the challenges is the large number of clothes so that they can observe hijab in the family and the society.
Hesitation in accepting occupational therapy philosophy
One of the important philosophies of occupational therapy revolves around using occupation and activity to treat the patient’s disability. Most of these activities include self-care, work, and leisure. According to several reviewed studies, occupational therapists’ challenges in Islamic countries are the desire for treatments that have faster results, including aggressive approaches, drug therapy, or sports-based interventions, which are less common in occupational therapists.
Discussion
The findings of this study illuminate the relationship between cultural context and the occupational performance of clients undergoing occupational therapy. It is evident that people’s occupational performance unfolds within a special environment and context, shaped and colored by various factors in any given society.
The positive effects of Islamic culture represent crucial factors that improve clients’ performance. Occupational therapists can leverage these factors to increase the independence of their clients and support them. In Islamic countries, family members and their unison often support the disabled person and form a backbone for improving the skills of people with disabilities through family assistance. Disruption of this support network can seriously damage the rehabilitation program. From a religious perspective, all the orders of Islam protect the family. Our study findings were consistent with the study of Anoushka (2019). In his research, Islam was found to be an important aspect of the participants’ lives. Many people conduct their daily activities and plan their families based on deep faith in God and his ability to protect them. The Islamic beliefs of the research participants regarded God as the ultimate decision-maker. They believed God had determined birth, death, marriage, and even employment [38].
Islam helps clients in different ways. For example, Islamic commands protect the body, prevent diseases, and help reduce stress and anxiety. Saged et al. (2022) stated that the Islamic religion-based interventions would significantly lower levels of depression and anxiety among participants. Also, a significant improvement in the patient’s general health was observed after the intervention. The participants were satisfied and believed everything that happened to them was predestined [39].
One of the important categories regarding positive opportunities to improve movement and other daily life skills is to observe prayers, which are highly valued in Islamic countries. Occupational therapists can use this opportunity to implement targeted skills and activities. The effects of prayer can be examined in various fields, for example, motor skills, brain activity, and other documented health benefits in multiple articles [40, 41, 42].
Cultural challenges pose obstacles to providing occupational therapy services, which must be dealt with delicately and require appropriate solutions. One of the cultural challenges is the respect for the principle of Mahram in interpersonal communication. Our findings were consistent with Caroline Murray’s study. From her point of view, the structure of social and cultural challenges, such as the social behaviors of occupational therapists and their norms, values, and beliefs, are vital [43].
Another important challenge in the treatment and rehabilitation of occupational therapy of clients revolves around certain beliefs about the cause of illness, which can create a serious challenge in providing services. Superstitious beliefs are rooted in factors such as a lack of awareness of natural events, environmental control, or fatalistic thinking [45].
The next challenge is the problems and limitations associated with prayers. This challenge, in some ways, may require a lot of effort and struggle on the part of clients or caregivers. It is stated in the Islamic rulings that prayer remains valid under any circumstances [46]. Ravari et al. highlighted that the failure of patients to pray may be due to the conditions of the hospital and related obstacles. These obstacles include the preparations for prayer, the patient’s movement status, and disease-related factors. Based on his study, patients who were aware of prayer rules during illness were more successful in performing the prayer [48].
The next challenge is doubt in accepting occupational therapy philosophy. As mentioned, a very important factor that determines people’s occupational performance is the environmental context that governs that society. In occupational therapy, this context is also an inevitable and effective factor in service delivery [49]. Considering that Iran has a special environmental context and due to this problem and some implementation problems, the use of occupation-based methods faces problems. Thus, clients and therapists prefer body function and structure-based methods due to the objectiveness of goals [50, 51]. A study conducted by Raji et al (2019) in Iran concluded that Iranian occupational therapists prioritized body function in children with cerebral palsy, with the activities of daily living and participation in society as their next priorities [52].
Many cultural challenges are due to the lack of a suitable cultural model based on the Islamic culture of Muslim countries. Actually, one of the appropriate solutions to these challenges can be study and research in this field. Additionally, strengthening the clinical reasoning of occupational therapists can be another useful step in this matter [43].
Conclusion
According to the analysis of the data obtained from the review of the articles, it is evident that Islam, a unique culture in Islamic countries, exerts profound effects on the daily life of occupational therapy clients. These effects can contribute positively and unite families during crises and illness. They also encompass the power of positive thoughts and recommendations to protect and support the disabled person. However, a series of challenges may cause obstacles in people’s daily lives and can even disrupt the treatment and rehabilitation of clients. Occupational therapists can employ these cultural opportunities to improve clients’ performance. Altogether, much research should be conducted to find a suitable model that occupational therapists employ for clinical reasoning to solve these challenges.
Ethical Considerations
Compliance with ethical guidelines
This article is a Meta synthesis with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, data analysis, writing, editing & review: All authors; Data collection: Hassan Vahidi and Nazila Akbar Fahimi; Supervision: Nazila Akbar Fahimi.
Conflict of interest
The authors declared no conflict of interest.
References
- Chiang M, Carlson G. Occupational therapy in multicultural contexts: Issues and strategies. British Journal of Occupational Therapy. 2003; 66(12):559-67. [DOI:10.1177/030802260306601204]
- Awaad J. Culture, cultural competency and occupational therapy: A review of the literature. British Journal of Occupational Therapy. 2003; 66(8):356-62. [DOI:10.1177/030802260306600804]
- Mumford D. Transcultural aspects of rehabilitation. In: Hume C, Pullen IM, editors. Rehabilitation for mental health problems: An introductory handbook. London: Churchill Livingstone; 1994. [Link]
- Moghadam VM. Modernizing women: Gender and social change in the Middle East. Colorado: Lynne Rienner Publishers; 2003. [DOI:10.1515/9781685858995]
- Bowen DL, Early EA. Everyday life in the Muslim Middle East: Indiana: Indiana University Press; 2002. [Link]
- Ahmad M, Khan S. A model of spirituality for ageing Muslims. Journal of Religion and Health. 2016; 55(3):830-43. [DOI:10.1007/s10943-015-0039-0] [PMID]
- Hagedorn R. Foundations for practice in occupational therapy: London: Churchill Livingstone; 1997. [Link]
- Iwama MK. Meaning and inclusion: Revisiting culture in occupational therapy. Australian Occupational Therapy Journal. 2004; 51(1):1-2. [DOI:10.1111/j.1440-1630.2004.00429.x]
- Kondo T. Cultural tensions in occupational therapy practice: Considerations from a Japanese vantage point. The American Journal of Occupational Therapy. 2004; 58(2):174-84. [DOI:10.5014/ajot.58.2.174] [PMID]
- Glen G, Brown ·C. Willard & Spackman’s occupational therapy. Pennsylvania: Wolters Kluwer Health; 2023. [Link]
- Rezaei M, Adib-Hajbaghery M, Seyedfatemi N, Hoseini F. Prayer in Iranian cancer patients undergoing chemotherapy. Complementary Therapies in Clinical Practice. 2008; 14(2):90-7. [DOI:10.1016/j.ctcp.2008.01.001] [PMID]
- Black RM. Intersections of care: An analysis of culturally competent care, client centered care, and the feminist ethic of care. Work. 2005; 24(4):409-22. [Link]
- Castro D, Dahlin-Ivanoff S, Mårtensson L. Occupational therapy and culture: A literature review. Scandinavian Journal of Occupational Therapy. 2014; 21(6):401-14. [DOI:10.3109/11038128.2014.898086] [PMID]
- Al Busaidy NS, Borthwick A. Occupational therapy in Oman: The impact of cultural dissonance. Occupational Therapy International. 2012; 19(3):154-64. [DOI:10.1002/oti.1332] [PMID]
- Awaad T. Culture, cultural competency and psychosocial occupational therapy: A Middle Eastern perspective. British Journal of Occupational Therapy. 2003; 66(9):409-13. [DOI:10.1177/030802260306600905]
- Malkawi SH, Alqatarneh NS, Fehringer EK. The influence of culture on occupational therapy practice in Jordan. Occupational Therapy International. 2020; 2020:1092805-. [DOI:10.1155/2020/1092805] [PMID]
- Maroney P, Potter M, Thacore VR. Experiences in occupational therapy with Afghan clients in Australia. Australian Occupational Therapy Journal. 2014; 61(1):13-9. [DOI:10.1111/1440-1630.12094] [PMID]
- Neuendorf KA. The content analysis guidebook. California: Sage Publications, Inc; 2017. [DOI:10.4135/9781071802878]
- Graneheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today. 2004; 24(2):105-12. [DOI:10.1016/j.nedt.2003.10.001] [PMID]
- Kassarjian HH. Content analysis in consumer research. Journal of Consumer Research. 1977; 4(1):8-18. [DOI:10.1086/208674]
- Mayring P. Qualitative content analysis. A Companion to Qualitative Research. 2004; 1(2):159-76. [Link]
- Mohamed CR, Nelson K, Wood P, Moss C. Issues post-stroke for Muslim people in maintaining the practice of salat (prayer): A qualitative study. Collegian. 2015; 22(3):243-9. [DOI:10.1016/j.colegn.2014.01.001] [PMID]
- Pooremamali P, Eklund M, Östman M, Persson D. Muslim Middle Eastern clients’ reflections on their relationship with their occupational therapists in mental health care. Scandinavian Journal of Occupational Therapy. 2012; 19(4):328-40. [DOI:10.3109/11038128.2011.600328] [PMID]
- Romli MH, Yunus FW. Malaysian occupational therapists’ perspective on prayer activity of Muslim clients. Education in Medicine Journal. 2016; 8(4):23-38. [DOI:10.5959/eimj.v8i4.448]
- Busuttil J. Establishing psychosocial occupational therapy in an Arab country. British Journal of Occupational Therapy. 1994; 57(4):124-6. [DOI:10.1177/030802269405700404]
- Busuttil J. Planning occupational therapy services in Kuwait. British Journal of Occupational Therapy. 1996; 59(3):125-7. [DOI:10.1177/030802269605900308]
- Engel-Yeger B. Comparing participation patterns in out-of-school activities between Israeli Jewish and Muslim children. Scandinavian Journal of Occupational Therapy. 2013; 20(5):323-35. [DOI:10.3109/11038128.2013.793738] [PMID]
- Thomas H. Developing a culturally competent model of occupational therapy in Bulgaria and Kosovo [BA thesis]. Carolina: University of North Carolina; 2017. [Link]
- Chowdhury N. Integration between mental health-care providers and traditional spiritual healers: Contextualising Islam in the twenty-first century. Journal of Religion and Health. 2016; 55(5):1665-71. [DOI:10.1007/s10943-016-0234-7] [PMID]
- Malone J, Dadswell A. The role of religion, spirituality and/or belief in positive ageing for older adults. Geriatrics. 2018; 3(2):28. [DOI:10.3390/geriatrics3020028] [PMID]
- Margolis SA, Carter T, Dunn EV, Reed RL. Validation of additional domains in activities of daily living, culturally appropriate for Muslims. Gerontology. 2003; 49(1):61-5. [DOI:10.1159/000066509] [PMID]
- Babaei M, Rassafiani M. [Scope of spirituality research in occupational therapy literature: A scoping review Study (Persian)]. Journal of Research in Rehabilitation Sciences. 2016; 12(3):185-93. [Link]
- Rassafiani M, Sahaf R, Yazdani F. Occupational therapy in Iran: Past, present, and future. Annals of International Occupational Therapy. 2018; 1(1):49-56. [DOI:10.3928/24761222-20180212-04]
- Babaei M, Rafiey H, Karbalaee-Nouri A, Rassafiani M, Haghgoo H, Biglarian A. Spirituality as a neglected core in occupational therapy practice: An Iranian Exploratory Survey. Journal of Religion and Health. 2023; 62(2):1207-22. [Link]
- Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Research Methods in Medicine & Health Sciences. 2020; 1(1):31-42. [DOI:10.1177/2632084320947559]
- Avenier MJ. Shaping a constructivist view of organizational design science. Organization Studies. 2010; 31(9-10):1229-55. [DOI:10.1177/0170840610374395]
- Mahrozade T, Shahi B. [The study of the Educational Nature of Critical thinking both From the Islamic View Point and Post Structuralism (Persian)]. Journal of Management and Planning in Educational Systems. 2013; 6(2):45-66. [Link]
- Ataullahjan A, Mumtaz Z, Vallianatos H. Family planning, Islam and sin: Understandings of moral actions in Khyber Pakhtunkhwa, Pakistan. Social Science & Medicine. 2019; 230:49-56. [DOI:10.1016/j.socscimed.2019.03.011] [PMID]
- Saged AAG, Sa'ari CZ, Abdullah MB, Al-Rahmi WM, Ismail WM, Zain MIA, et al. The effect of an Islamic-Based intervention on depression and anxiety in Malaysia. Journal of Religion and Health. 2022; 61(1):79-92. [DOI:10.1007/s10943-021-01484-3] [PMID]
- Chamsi-Pasha M, Chamsi-Pasha H. A review of the literature on the health benefits of Salat (Islamic prayer). The Medical Journal of Malaysia. 2021; 76(1):93-7. [PMID]
- Doufesh H, Ibrahim F, Safari M. Effects of Muslims praying (Salat) on EEG gamma activity. Complementary Therapies in Clinical Practice. 2016; 24:6-10. [DOI:10.1016/j.ctcp.2016.04.004] [PMID]
- Hamed Msed. Effect of regular prayer (SALAT) Movements on postural balance. Giza: Cairo University; 2012.
- Murray C, Turpin M, Edwards I, Jones M. A qualitative meta-synthesis about challenges experienced in occupational therapy practice. British Journal of Occupational Therapy. 2015; 78(9):534-46. [DOI:10.1177/0308022615586786]
- Taher M, Pashaeypoor S, Cheraghi MA, Karimy M, Hoseini ASS. Superstition in health beliefs: Concept exploration and development. Journal of Family Medicine and Primary Care. 2020; 9(3):1325-30. [DOI:10.4103/jfmpc.jfmpc_871_19] [PMID]
- Larose F, Bourque J, Freiman V. The effect of contextualising probability education on differentiating the concepts of luck, chance, and probabilities among middle and high school pupils in Quebec. Data and context in statistics education: Towards an evidence-based society Proceedings of the Eighth International Conference on Teaching Statistics. 2010; 1-4. [Link]
- Demehri F, Honarmand M, Yavari A. [Depression and obsessive-compulsive as antecedent of guilt feeling and anxiety as consequences of it in university girl students (Persian)]. Journal of Woman Cultural Psychology. 2011; 2(6):25-36. [Link]
- Kazemi M, Vazirinejad R, Ravari A, Jafarpor P. [Relationship between religious attitudes and prayer of patients in medical and surgical in Hospital of AliIbn AbiTaleb, Rafsanjan, 2012 (Persian)]. Community Health Journal. 2012; 6(3):31-8. [Link]
- Ravi A, Mirzaei T, Mirzaei S, Kazemi M, Hosieni F. [Prayer (Salat) performance for patient, patients, hospital (Persian)]. Journal of Medicine and Spiritual Cultivation. 2018; 26(2):145-58.
- Kondo T. Cultural tensions in occupational therapy practice: Considerations from a Japanese vantage point. American Journal of Occupational Therapy. 2004; 58(2):174-84. [DOI:10.5014/ajot.58.2.174] [PMID]
- Khayatzadeh Mahani M, Hassani Mehraban A, Kamali M, Parvizy S. Facilitators of implementing occupation based practice among Iranian occupational therapists: A qualitative study. Medical Journal of The Islamic Republic of Iran. 2015; 29:307. [PMID]
- Khazaeli K, Rassafiani M, Sourtiji H. [A study on employing occupation during intervention by occupational therapists in Isfahan and Tehran, Iran (Persian)]. Journal of Research in Rehabilitation Science. 2012; 8(1):132-44. [Link]
- Raji P, Mehraban AH, Ahmadi M, Schiariti V. Assessment priorities in cerebral palsy using ICF core set by Iranian occupational therapists. Canadian Journal of Occupational Therapy. 2019;86(4):289-98. [DOI:10.1177/0008417419833400] [PMID]
Type of Study: Systematic Review |
Subject:
Occupational Therapy
Received: 17/12/2022 | Accepted: 29/05/2023 | Published: 1/10/2023
Received: 17/12/2022 | Accepted: 29/05/2023 | Published: 1/10/2023
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
